Journal of International Oncology ›› 2025, Vol. 52 ›› Issue (9): 566-575.doi: 10.3760/cma.j.cn371439-20250417-00096
• Original Article • Previous Articles Next Articles
Prospective cohort study on the effect of abdominal circumference on the intestinal radiation dose volume and the acute intestinal toxicity in pelvic intensity modulated radiation therapy for rectal cancer patients
Wu Songyou1,2, Wang Gang1,2,3( ), Wang Wenling1,2,3, Dong Hongmin1,2,3, Chen Weiwei1,2,3, Li Xiaokai1,2,3, Chen Wanghua1,2,3, Zuo Kai1,2,3
), Wang Wenling1,2,3, Dong Hongmin1,2,3, Chen Weiwei1,2,3, Li Xiaokai1,2,3, Chen Wanghua1,2,3, Zuo Kai1,2,3
- 1Department of Oncology, Clinical Medical College of Guizhou Medical University, Guiyang 550004, China
2Department of Abdominal Oncology, Affiliated Cancer Hospital of Guizhou Medical University, Guiyang 550008, China
3Department of Oncology, Affiliated Hospital of Guizhou Medical University, Guiyang 550001, China
-
Received:2025-04-17Revised:2025-05-18Online:2025-09-08Published:2025-10-21 -
Contact:Wang Gang E-mail:389896586@qq.com -
Supported by:Science and Technology Program of Guizhou Province Anti-Cancer Association(Kang Xie Ke Ji 010 〔2023〕)
Cite this article
Wu Songyou, Wang Gang, Wang Wenling, Dong Hongmin, Chen Weiwei, Li Xiaokai, Chen Wanghua, Zuo Kai. Prospective cohort study on the effect of abdominal circumference on the intestinal radiation dose volume and the acute intestinal toxicity in pelvic intensity modulated radiation therapy for rectal cancer patients[J]. Journal of International Oncology, 2025, 52(9): 566-575.
share this article
"
| 一般临床资料 | 辅助放疗(n=82) | 新辅助放疗(n=68) |
|---|---|---|
| 年龄 | 57.33±11.13 | 53.72±9.68 |
| 性别 | ||
| 女 | 29 | 22 |
| 男 | 53 | 46 |
| 身高(cm) | 160.99±7.76 | 160.69±7.00 |
| 体质量(kg) | 57.59±10.18 | 58.48±10.06 |
| BMI(kg/m2) | 22.17±3.26 | 22.63±3.56 |
| 腹围(cm) | 80.85±8.03 | 80.67±8.70 |
| T分期 | ||
| T1 | 1 | 0 |
| T2 | 4 | 2 |
| T3 | 65 | 32 |
| T4 | 12 | 34 |
| N分期 | ||
| N0 | 35 | 5 |
| N1 | 28 | 23 |
| N2 | 19 | 40 |
| 直肠病灶位置 | ||
| 上段 | 20 | 10 |
| 中段 | 39 | 29 |
| 下段 | 23 | 29 |
| PTV(cm3) | 11.39±1.50 | 11.31±1.79 |
| 肠道体积(cm3) | 8.05±3.13 | 8.09±3.52 |
| 膀胱体积(cm3) | 2.64(2.05,3.47) | 2.53(1.95,2.88) |
| 急性肠道毒性(级) | ||
| <2 | 59 | 51 |
| ≥2 | 23 | 17 |
"
| 因素 | V10 | V20 | V30 | V40 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | ||||
| 年龄 | 0.34 | -0.20~0.87 | 0.213 | 0.09 | -0.20~0.38 | 0.540 | 0.10 | -0.10~0.29 | 0.319 | 0.07 | -0.07~0.21 | 0.337 | |||
| 性别 | -24.93 | -36.03~13.82 | <0.001 | -13.43 | -19.51~7.34 | <0.001 | -7.72 | -11.84~3.59 | <0.001 | -5.62 | -8.65~2.60 | <0.001 | |||
| 身高 | -0.76 | -1.51~0.01 | 0.049 | -0.41 | -0.82~0.01 | 0.049 | -0.25 | -0.52~0.03 | 0.075 | -0.19 | -0.39~0.01 | 0.057 | |||
| 体质量 | -0.78 | -1.34~-0.22 | 0.007 | -0.65 | -0.94~-0.37 | <0.001 | -0.41 | -0.60~-0.22 | <0.001 | -0.30 | -0.44~-0.17 | <0.001 | |||
| BMI | -1.68 | -3.45~0.09 | 0.063 | -1.77 | -2.68~0.86 | <0.001 | -1.11 | -1.71~-0.50 | <0.001 | -0.82 | -1.26~-0.38 | <0.001 | |||
| 腹围 | -0.77 | -1.49~0.05 | 0.037 | -0.78 | -1.15~-0.41 | <0.001 | -0.49 | -0.73~-0.25 | <0.001 | -0.37 | -0.55~-0.19 | <0.001 | |||
| T分期 | -3.20 | -15.33~8.93 | 0.601 | -1.80 | -8.43~4.82 | 0.590 | -1.61 | -5.97~2.75 | 0.464 | -1.61 | -4.80~1.57 | 0.316 | |||
| N分期 | 2.73 | -4.78~10.24 | 0.472 | -1.42 | -5.52~2.68 | 0.493 | -1.38 | -4.07~1.32 | 0.312 | -0.79 | -2.77~1.19 | 0.430 | |||
| 直肠病灶 位置 | 1.40 | -6.80~9.60 | 0.734 | 3.14 | -1.29~7.57 | 0.162 | 2.68 | -0.22~5.57 | 0.069 | 2.01 | -0.11~4.12 | 0.063 | |||
| PTV | 0.73 | 0.37~1.10 | <0.001 | 0.37 | 0.17~0.57 | <0.001 | 0.21 | 0.07~0.34 | 0.003 | 0.12 | 0.02~0.22 | 0.018 | |||
| 肠道体积 | 0.82 | 0.76~0.82 | <0.001 | 0.36 | 0.29~0.42 | <0.001 | 0.21 | 0.16~0.26 | <0.001 | 0.15 | 0.12~0.19 | <0.001 | |||
| 膀胱体积 | 0.53 | -0.14~1.20 | 0.118 | 0.01 | -0.36~0.38 | 0.964 | 0.05 | -0.19~0.30 | 0.672 | 0.07 | -0.11~0.24 | 0.469 | |||
"
| 因素 | V10 | V20 | V30 | V40 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | ||||
| 年龄 | 0.32 | -0.34~0.97 | 0.340 | 0.19 | -0.10~0.48 | 0.195 | 0.10 | -0.06~0.25 | 0.217 | 0.06 | -0.05~0.17 | 0.298 | |||
| 性别 | -18.44 | -31.20~-5.68 | 0.005 | -3.78 | -9.76~2.20 | 0.211 | -8.85 | -4.04~2.34 | 0.598 | -0.65 | -2.94~1.64 | 0.574 | |||
| 身高 | -0.78 | -1.67~0.11 | 0.084 | -0.29 | -0.62~0.19 | 0.071 | -0.05 | -0.27~0.17 | 0.643 | -0.01 | -0.16~0.15 | 0.954 | |||
| 体质量 | -0.64 | -1.26~-0.03 | 0.041 | -0.52 | -0.77~-0.27 | <0.001 | -0.25 | -0.39~-0.11 | 0.001 | -0.19 | -0.28~-0.16 | <0.001 | |||
| BMI | -1.09 | -2.86~0.69 | 0.226 | -1.36 | -2.09~-0.64 | <0.001 | -0.71 | -1.10~-0.33 | <0.001 | -0.56 | -0.84~-0.29 | <0.001 | |||
| 腹围 | -0.81 | -1.51~-0.10 | 0.026 | -0.74 | -1.01~-0.47 | <0.001 | -0.37 | -0.52~-0.23 | <0.001 | -0.28 | -0.38~-0.17 | <0.001 | |||
| T分期 | -7.84 | -19.09~3.42 | 0.169 | -2.40 | -7.47~2.67 | 0.348 | -1.95 | -4.60~0.70 | 0.146 | -1.82 | -3.71~0.06 | 0.057 | |||
| N分期 | 0.75 | -9.31~10.81 | 0.882 | -0.01 | -4.51~4.49 | 0.996 | -0.39 | -2.76~1.98 | 0.742 | 0.01 | -1.70~1.71 | 0.993 | |||
| 直肠病灶 位置 | 4.01 | -4.93~12.96 | 0.374 | 2.04 | -1.95~6.03 | 0.311 | 1.60 | -0.48~3.69 | 0.130 | 1.48 | 0.00~2.97 | 0.050 | |||
| PTV | 0.03 | -0.33~0.39 | 0.874 | 0.02 | -0.14~0.18 | 0.775 | 0.01 | -0.08~0.09 | 0.822 | 0.01 | -0.07~0.05 | 0.708 | |||
| 肠道体积 | 0.66 | 0.58~0.74 | <0.001 | 0.21 | 0.14~0.27 | <0.001 | 0.10 | 0.06~0.13 | <0.001 | 0.07 | 0.04~0.10 | <0.001 | |||
| 膀胱体积 | 0.18 | -0.42~0.77 | 0.556 | -0.14 | -0.40~0.13 | 0.310 | -0.08 | -0.22~0.06 | 0.257 | -0.04 | -0.14~0.06 | 0.475 | |||
"
| 因素 | 辅助放疗(n=82) | 新辅助放疗(n=68) | |||||
|---|---|---|---|---|---|---|---|
| OR值 | 95%CI | P值 | OR值 | 95%CI | P值 | ||
| 年龄 | 0.99 | 0.95~1.03 | 0.586 | 0.97 | 0.92~1.03 | 0.281 | |
| 性别 | 0.80 | 0.30~2.16 | 0.656 | 1.20 | 0.36~3.96 | 0.765 | |
| 身高 | 0.99 | 0.93~1.06 | 0.855 | 1.01 | 0.93~1.09 | 0.864 | |
| 体质量 | 0.95 | 0.90~1.00 | 0.054 | 0.94 | 0.89~1.00 | 0.016 | |
| BMI | 0.83 | 0.70~0.98 | 0.028 | 0.82 | 0.68~0.99 | 0.037 | |
| 腹围 | 0.90 | 0.83~0.97 | 0.004 | 0.89 | 0.82~0.97 | 0.007 | |
| T分期 | 1.41 | 0.51~3.88 | 0.509 | 0.78 | 0.29~2.07 | 0.614 | |
| N分期 | 1.27 | 0.69~2.34 | 0.439 | 1.05 | 0.44~2.53 | 0.912 | |
| 直肠病灶位置 | 0.81 | 0.41~1.58 | 0.532 | 1.04 | 0.48~2.28 | 0.921 | |
| PTV | 1.00 | 0.97~1.03 | 0.850 | 1.00 | 0.97~1.03 | 0.948 | |
| 肠道体积 | 1.02 | 1.00~1.04 | 0.024 | 1.00 | 0.99~1.02 | 0.768 | |
| 膀胱体积 | 1.03 | 0.98~1.09 | 0.276 | 1.02 | 0.97~1.07 | 0.523 | |
| V10 | 1.03 | 1.01~1.05 | 0.007 | 1.01 | 0.99~1.03 | 0.236 | |
| V20 | 1.05 | 1.01~1.09 | 0.006 | 1.08 | 1.02~1.15 | 0.009 | |
| V30 | 1.08 | 1.02~1.14 | 0.007 | 1.14 | 1.03~1.27 | 0.015 | |
| V40 | 1.11 | 1.03~1.19 | 0.007 | 1.16 | 1.02~1.31 | 0.025 | |
"
| 因素 | 辅助放疗(n=82) | 新辅助放疗(n=68) | |||||
|---|---|---|---|---|---|---|---|
| β值 | 95%CI | P值 | β值 | 95%CI | P值 | ||
| V10 | |||||||
| 未调整 | -0.77 | -1.49~-0.05 | 0.037 | -0.81 | -1.51~-0.10 | 0.026 | |
| 模型Ⅰ | -1.01 | -1.68~-0.33 | 0.004 | -0.92 | -1.62~-0.22 | 0.010 | |
| V20 | |||||||
| 未调整 | -0.78 | -1.15~-0.41 | <0.001 | -0.74 | -1.01~-0.47 | <0.001 | |
| 模型Ⅰ | -0.94 | -1.28~-0.60 | <0.001 | -0.84 | -1.11~-0.57 | <0.001 | |
| V30 | |||||||
| 未调整 | -0.49 | -0.73~-0.25 | <0.001 | -0.37 | -0.52~-0.23 | <0.001 | |
| 模型Ⅰ | -0.58 | -0.82~-0.34 | <0.001 | -0.42 | -0.57~-0.28 | <0.001 | |
| V40 | |||||||
| 未调整 | -0.37 | -0.55~-0.19 | <0.001 | -0.28 | -0.38~-0.17 | <0.001 | |
| 模型Ⅰ | -0.41 | -0.60~-0.23 | <0.001 | -0.30 | -0.41~-0.19 | <0.001 | |
"
| 因素 | 辅助放疗(n=82) | 新辅助放疗(n=68) | |||||
|---|---|---|---|---|---|---|---|
| OR值 | 95%CI | P值 | OR值 | 95%CI | P值 | ||
| 未调整 | 0.90 | 0.83~0.97 | 0.004 | 0.89 | 0.82~0.97 | 0.007 | |
| 模型Ⅰ | 0.86 | 0.78~0.95 | 0.002 | 0.87 | 0.79~0.96 | 0.004 | |
"
"
| 项目 | V10 | V20 | V30 | V40 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | ||||
| 一条直线效应 | -1.01 | -1.68~-0.33 | 0.004 | -0.94 | -1.28~-0.60 | <0.001 | -0.58 | -0.82~-0.34 | <0.001 | -0.41 | -0.60~-0.23 | <0.001 | |||
| 拐点(cm) | 71.9 | 71.9 | 71.9 | 71.9 | |||||||||||
| <拐点值 | 2.87 | -0.66~6.39 | 0.115 | 1.00 | -0.77~2.76 | 0.271 | 1.04 | -0.21~2.30 | 0.108 | 0.71 | -0.23~1.66 | 0.144 | |||
| >拐点值 | -1.42 | -2.16~-0.67 | <0.001 | -1.15 | -1.52~-0.77 | <0.001 | -0.79 | -1.02~-0.48 | <0.001 | -0.53 | -0.73~-0.33 | <0.001 | |||
| 对数似然比检验 | 0.022 | 0.022 | 0.008 | 0.013 | |||||||||||
"
| 项目 | V10 | V20 | V30 | V40 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | β值 | 95%CI | P值 | ||||
| 一条直线效应 | -0.92 | -1.62~-0.22 | <0.010 | -0.84 | -1.11~-0.57 | <0.001 | -0.42 | -0.57~-0.28 | <0.001 | -0.30 | -0.41~-0.19 | <0.001 | |||
| 拐点(cm) | 69.0 | 69.0 | 69.0 | 68.6 | |||||||||||
| <拐点值 | 3.31 | -5.94~12.56 | 0.486 | 0.21 | -3.32~3.74 | 0.906 | 0.42 | -1.52~2.37 | 0.671 | 0.55 | -1.06~2.16 | 0.508 | |||
| >拐点值 | -1.06 | -1.78~-0.33 | 0.006 | -0.88 | -1.16~-0.61 | <0.001 | -0.45 | -0.61~-0.30 | <0.001 | -0.32 | -0.43~-0.21 | <0.001 | |||
| 对数似然比检验 | 0.333 | 0.523 | 0.355 | 0.267 | |||||||||||
"
"
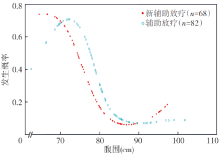
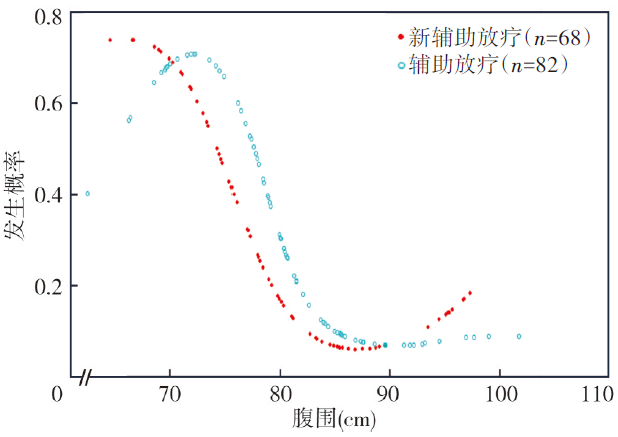
| 项目 | 辅助放疗(n=82) | 新辅助放疗(n=68) | |||||
|---|---|---|---|---|---|---|---|
| OR值 | 95%CI | P值 | OR值 | 95%CI | P值 | ||
| 一条直线效应 | 0.86 | 0.78~0.95 | 0.002 | 0.87 | 0.79~0.96 | 0.004 | |
| 拐点 | 71.9 | 69.0 | |||||
| <拐点值 | 1.33 | 0.84~2.08 | 0.220 | 2.20 | 0.70~6.90 | 0.176 | |
| >拐点值 | 0.78 | 0.67~0.90 | <0.001 | 0.60 | 0.42~ 0.85 | 0.004 | |
| 对数似然比检验 | 0.022 | 0.033 | |||||
| 拐点值95%CI | 69.2~76.1 | 66.7~71.9 | |||||
"
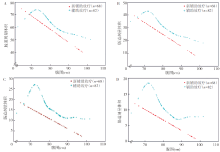
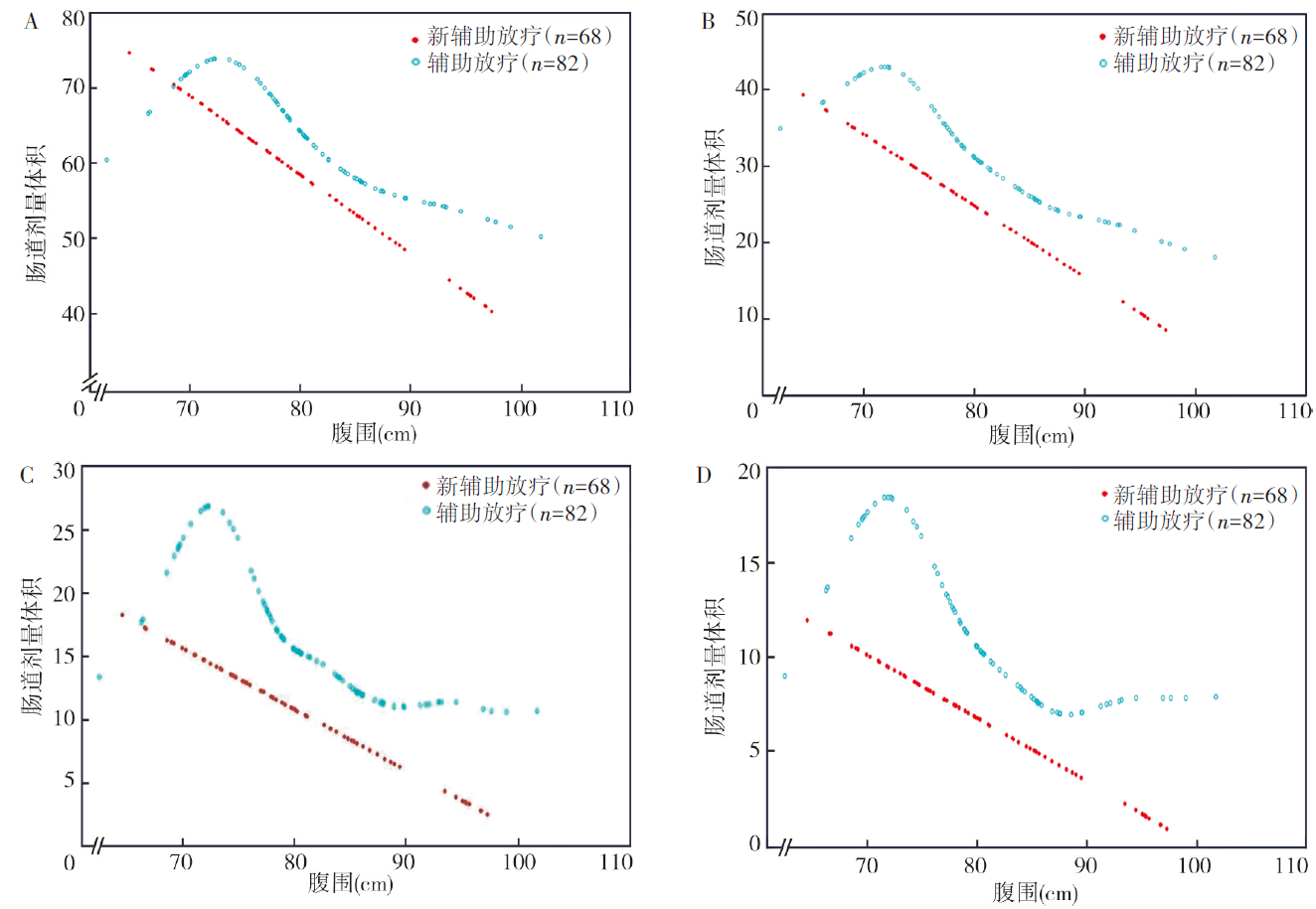
| 肠道受照 剂量体积 | 辅助放疗 | 新辅助放疗 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 小腹围(n=22) | 中大腹围(n=60) | t值 | P值 | 小腹围(n=11) | 中大腹围(n=57) | t/Z值 | P值 | ||
| V10 | 7.65±2.29 | 5.88±2.68 | 2.76 | 0.007 | 6.82±3.01 | 5.58±2.49 | 1.47 | 0.147 | |
| V20 | 4.28±1.27 | 2.72±1.31 | 4.81 | <0.001 | 3.09±0.84 | 2.28±1.17 | 2.17 | 0.033 | |
| V30 | 2.42±1.07 | 1.37±0.76 | 4.95 | <0.001 | 1.44(1.22,1.53) | 0.91(0.56,1.22) | -3.04 | 0.002 | |
| V40 | 1.69±0.74 | 0.92±0.58 | 4.93 | <0.001 | 0.93(0.84,1.09) | 0.44(0.30,0.81) | -3.19 | 0.001 | |
"
| 急性肠道 毒性等级 | 辅助放疗 | 新辅助放疗 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 小腹围(n=22) | 中大腹围(n=60) | χ2值 | P值 | 小腹围(n=11) | 中大腹围(n=57) | χ2值 | P值 | ||
| <2级 | 10 | 49 | 10.46 | 0.001 | 4 | 47 | 8.13 | 0.004 | |
| ≥2级 | 12 | 11 | 7 | 10 | |||||
| [1] | Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74(3): 229-263. DOI: 10.3322/caac.21834. |
| [2] | 王裕新, 潘凯枫, 李文庆. 2022全球癌症统计报告解读[J]. 肿瘤综合治疗电子杂志, 2024, 10(3): 1-16. DOI: 10.12151/JMCM.2024.03-01. |
| [3] | 国家卫生健康委员会医政司, 中华医学会肿瘤学分会. 国家卫健委中国结直肠癌诊疗规范(2023版)[J]. 中国实用外科杂志, 2023, 43(6): 602-630. DOI: 10.19538/j.cjps.issn1005-2208.2023.06.02. |
| [4] | Benson AB, Venook AP, Adam M, et al. NCCN guidelines® insights: rectal cancer, version 3.2024[J]. J Natl Compr Canc Netw, 2024, 22(6): 366-375. DOI: 10.6004/jnccn.2024.0041. |
| [5] | Hale MF. Radiation enteritis: from diagnosis to management[J]. Curr Opin Gastroenterol, 2020, 36(3): 208-214. DOI: 10.1097/MOG.0000000000000632. |
| [6] | Samuelian JM, Callister MD, Ashman JB, et al. Reduced acute bowel toxicity in patients treated with intensity-modulated radiotherapy for rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2012, 82(5): 1981-1987. DOI: 10.1016/j.ijrobp.2011.01.051. |
| [7] | Baglan KL, Frazier RC, Yan D, et al. The dose-volume relationship of acute small bowel toxicity from concurrent 5-FU-based chemotherapy and radiation therapy for rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2002, 52(1): 176-183. DOI: 10.1016/s0360-3016(01)01820-x. |
| [8] | Robertson JM, Lockman D, Yan D, et al. The dose-volume relationship of small bowel irradiation and acute grade 3 diarrhea during chemoradiotherapy for rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2008, 70(2): 413-418. DOI: 10.1016/j.ijrobp.2007.06.066. |
| [9] |
Kim JY, Kim DY, Kim TH, et al. Intensity-modulated radiotherapy with a belly board for rectal cancer[J]. Int J Colorectal Dis, 2007, 22(4): 373-379. DOI: 10.1007/s00384-006-0166-x.
pmid: 16802067 |
| [10] |
Wo JY, Anker CJ, Ashman JB, et al. Radiation therapy for rectal cancer: executive summary of an ASTRO clinical practice guideline[J]. Pract Radiat Oncol, 2021, 11(1): 13-25. DOI: 10.1016/j.prro.2020.08.004.
pmid: 33097436 |
| [11] | Wang G, Wang W, Jin H, et al. Effect of abdominal circumference on the irradiated bowel volume in pelvic radiotherapy for rectal cancer patients: implications for the radiotherapy-related intestinal toxicity[J]. Front Oncol, 2022, 12: 843704. DOI: 10.3389/fonc.2022.843704. |
| [12] | Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC)[J]. Int J Radiat Oncol Biol Phys, 1995, 31(5):1341-1346. DOI: 10.1016/0360-3016(95)00060-C. |
| [13] |
Nijkamp J, Doodeman B, Marijnen C, et al. Bowel exposure in rectal cancer IMRT using prone, supine, or a belly board[J]. Radiother Oncol, 2012, 102(1): 22-29. DOI: 10.1016/j.radonc.2011.05.076.
pmid: 21723637 |
| [14] |
Yang Y, Cai S, Zhao T, et al. Effect of prone and supine treatment positions for postoperative treatment of rectal cancer on target dose coverage and small bowel sparing using intensity-modulated radiation therapy[J]. Transl Cancer Res, 2020, 9(2): 491-499. DOI: 10.21037/tcr.2019.11.33.
pmid: 35117393 |
| [15] |
Scobioala S, Kittel C, Niermann P, et al. A treatment planning study of prone vs. supine positions for locally advanced rectal carcinoma: comparison of 3‑dimensional conformal radiotherapy, tomotherapy, volumetric modulated arc therapy, and intensity-modulated radiotherapy[J]. Strahlenther Onkol, 2018, 194(11): 975-984. DOI: 10.1007/s00066-018-1324-0.
pmid: 29855667 |
| [16] |
Holyoake DLP, Partridge M, Hawkins MA. Systematic review and meta-analysis of small bowel dose-volume and acute toxicity in conventionally-fractionated rectal cancer radiotherapy[J]. Radiother Oncol, 2019, 138: 38-44. DOI: 10.1016/j.radonc.2019.05.001.
pmid: 31136961 |
| [17] |
Roeske JC, Bonta D, Mell LK, et al. A dosimetric analysis of acute gastrointestinal toxicity in women receiving intensity-modulated whole-pelvic radiation therapy[J]. Radiother Oncol, 2003, 69(2): 201-207. DOI: 10.1016/j.radonc.2003.05.001.
pmid: 14643959 |
| [18] |
Sini C, Noris Chiorda B, Gabriele P, et al. Patient-reported intestinal toxicity from whole pelvis intensity-modulated radiotherapy: first quantification of bowel dose-volume effects[J]. Radiother Oncol, 2017, 124(2): 296-301. DOI: 10.1016/j.radonc.2017.07.005.
pmid: 28739383 |
| [19] |
Lee J, Chang CL, Lin JB, et al. The effect of body mass index and weight change on late gastrointestinal toxicity in locally advanced cervical cancer treated with intensity-modulated radiotherapy[J]. Int J Gynecol Cancer, 2018, 28(7): 1377-1386. DOI: 10.1097/IGC.0000000000001312.
pmid: 29994908 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||