国际肿瘤学杂志 ›› 2021, Vol. 48 ›› Issue (3): 150-155.doi: 10.3760/cma.j.cn371439-20200409-00030
徐士飞1,2, 冯欢1, 刘海洋2, 胡杰2, 马露1
Xu Shifei1,2, Feng Huan1, Liu Haiyang2, Hu Jie2, Ma Lu1
摘要:
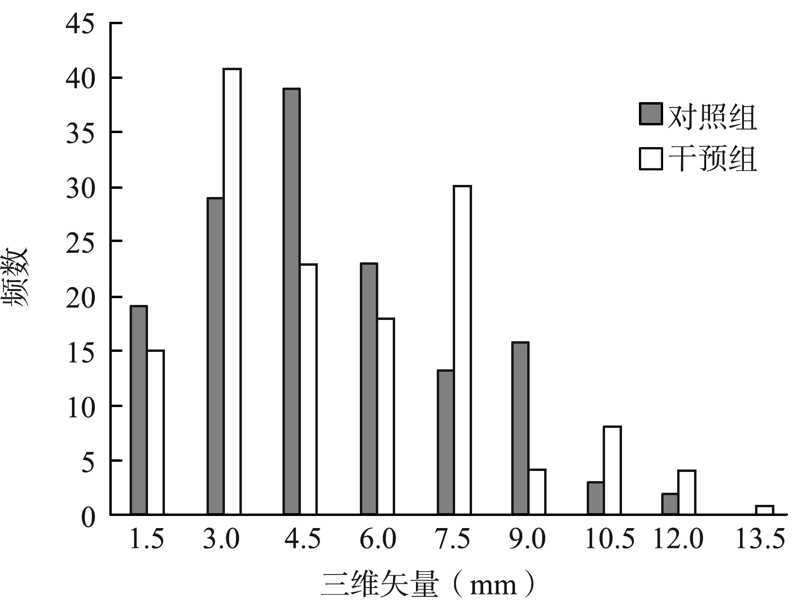
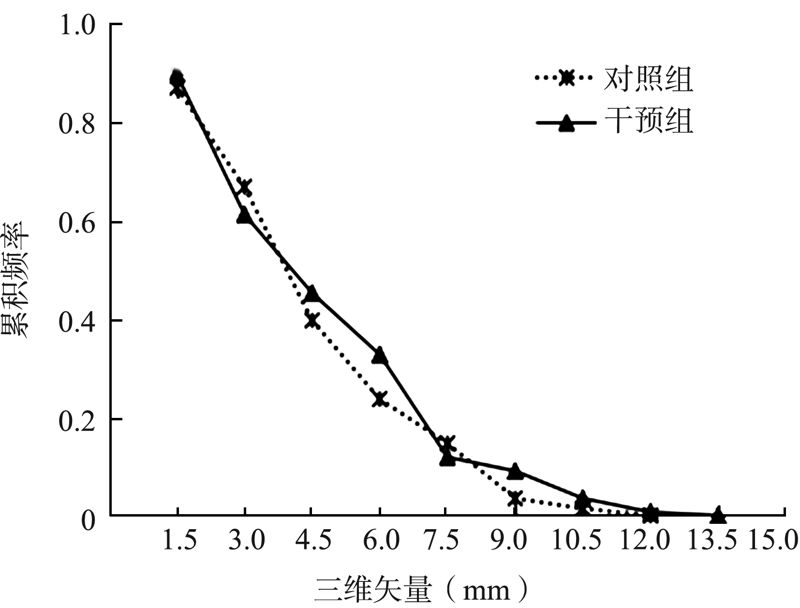
目的 研究头颈部肿瘤旋转误差对放疗位置精准性(PA)的影响,评价是否需要矫正旋转误差。方法 收集2019年8月至2020年1月武汉大学中南医院肿瘤放疗中心34例头颈部肿瘤患者的图像资料。每例患者放疗前拍摄兆伏级计算机断层扫描(MVCT)图像,采用两种配准方式与计划千伏级计算机断层扫描(KVCT)图像配准,根据不同配准方式分为对照组(平移配准)和干预组(平移和旋转配准),两组各有144次图像配准。记录两种配准方式的位置误差并比较。数据处理采用Wilcoxon符号秩检验和Spearman秩相关分析。结果 对照组和干预组左右方向平移误差分别为0.10(5.35)mm和0.00(5.78)mm,差异有统计学意义(Z=-2.675,P=0.007);上下方向分别为0.75(2.78)mm和0.60(2.68)mm,差异有统计学意义(Z=-2.819,P=0.005);前后方向分别为0.10(0.90)mm和0.20(1.28)mm,差异有统计学意义(Z=-3.984,P<0.001)。干预组俯仰角(pitch)、翻滚角(roll)、偏航角(yaw)旋转误差分别为-0.20(0.60)°、0.35(2.00)°和0.00(0.98)°。两组三维矢量矫正频数呈正偏态分布。矫正累积频率(CCF)随三维矢量不同而变化,三维矢量为8.0 mm,对照组和干预组分别有19次和16次分次治疗未矫正;三维矢量在8.0~13.5 mm之间,干预组矫正趋势减缓且延迟矫正全部分次治疗。Spearman秩相关分析显示,pitch旋转误差与对照组上下方向和干预组前后方向平移误差均呈负相关(r=-0.182,P=0.029和r=-0.484,P<0.001);roll旋转误差与干预组左右方向平移误差呈负相关(r=-0.334,P<0.001);yaw旋转误差与对照组上下方向平移误差呈负相关(r=-0.171,P=0.040),yaw旋转误差与干预组左右和上下方向平移误差分别呈正相关(r=0.370,P<0.001)和负相关(r=-0.203,P=0.015);总角度与对照组上下、前后方向平移误差和三维矢量分别呈正相关(r=0.246,P=0.003)、负相关(r=-0.188,P=0.024)和正相关(r=0.198,P=0.017),总角度与干预组上下方向平移误差和三维矢量均呈正相关(r=0.170,P=0.041;r=0.239,P=0.004);其余变量间均无相关性(均P>0.05)。结论 尽管矫正旋转增加前后方向平移误差和三维矢量,但可促进头颈部肿瘤放疗PA。旋转矫正受限可通过矫正平移误差补偿,以降低其对PA的影响。