国际肿瘤学杂志 ›› 2021, Vol. 48 ›› Issue (3): 156-163.doi: 10.3760/cma.j.cn371439-20201116-00031
宋扬, 王斌*( ), 肖何, 陈川, 王阁, 耿明英
), 肖何, 陈川, 王阁, 耿明英
Song Yang, Wang Bin*(), Xiao He, Chen Chuan, Wang Ge, Geng Mingying
摘要:
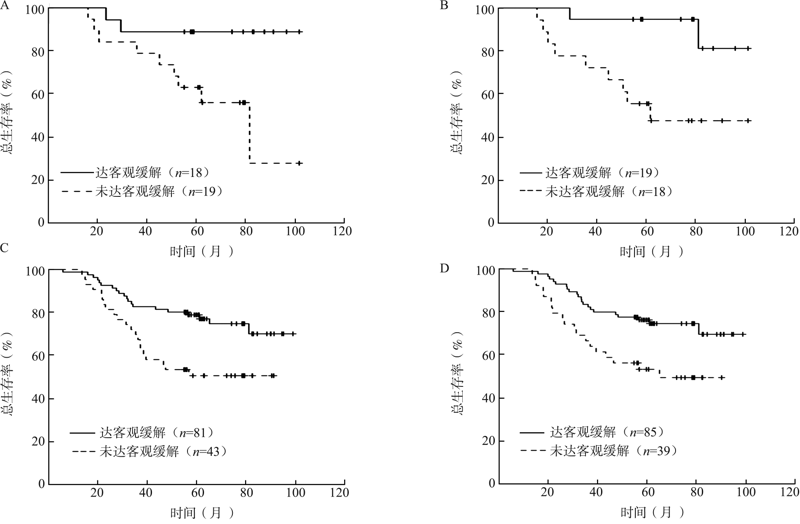
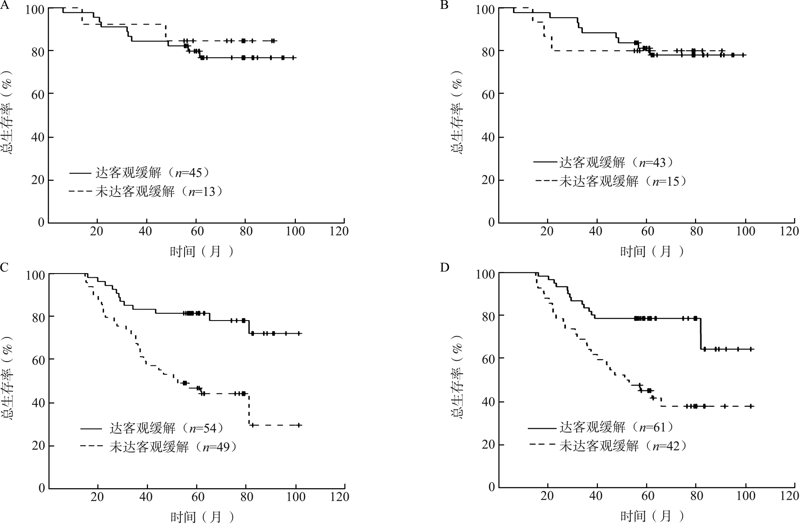
目的 探讨局部晚期鼻咽癌诱导化疗后肿瘤退缩率对生存预后的预测价值。方法 选择2009年1月至2012年12月在陆军军医大学大坪医院初治的161例Ⅲ~ⅣA期鼻咽癌患者作为研究对象,分析鼻咽癌患者诱导化疗前后肿瘤体积变化与患者生存时间的关系。采用Kaplan-Meier法绘制生存曲线并行log-rank检验,采用Cox回归分析影响鼻咽癌患者预后的危险性因素。结果 鼻咽原发肿瘤诱导化疗后肿瘤退缩率在N2-3期和N1期(Z=2.177,P=0.029)及T1-2期和T3-4期(Z=-4.501,P<0.001)患者间差异均有统计学意义。在N1期患者中,诱导化疗后鼻咽原发肿瘤达到(n=18)与未达到客观缓解患者(n=19)的5年总生存(OS)率分别为88.89%、57.45%,颈部淋巴结转移肿瘤达到(n=19)与未达到客观缓解患者(n=18)的5年OS率分别为86.72%、49.10%,差异均有统计学意义(χ 2=6.023,P=0.014;χ 2=7.441,P=0.006);N2-3期患者中,诱导化疗后鼻咽原发肿瘤达到(n=81)和未达到客观缓解患者(n=43)的5年OS率分别为77.56%、50.70%,颈部淋巴结转移肿瘤达到(n=85)与未达到客观缓解患者(n=39)的5年OS率分别为75.11%、52.04%,差异均有统计学意义(χ 2=8.037,P=0.005;χ 2=7.268,P=0.007)。单因素Cox回归分析表明,在N1期患者中,诱导化疗后鼻咽原发肿瘤退缩率(HR=0.048,95%CI为0.004~0.644,P=0.022)、鼻咽原发肿瘤疗效(HR=0.174,95%CI为0.037~0.830,P=0.028)和颈部淋巴结转移肿瘤疗效(HR=0.154,95%CI为0.033~0.725,P=0.017)均与OS相关;在N2-3期患者中,诱导化疗后鼻咽原发肿瘤退缩率(HR=0.178,95%CI为0.056~0.564,P=0.003)、颈部淋巴结转移肿瘤退缩率(HR=0.081,95%CI为0.020~0.324,P<0.001)、鼻咽原发肿瘤疗效(HR=0.422,95%CI为0.228~0.781,P=0.006)和颈部淋巴结转移肿瘤疗效(HR=0.439,95%CI为0.238~0.813,P=0.009)均与OS相关;在包含N分期和肿瘤退缩率以及N分期和疗效的多因素Cox回归中,交互项均未达到统计学意义(均P>0.05)。在T1-2期患者中,诱导化疗后鼻咽原发肿瘤达到(n=45)与未达到客观缓解患者(n=13)的5年OS率分别为77.55%、84.62%,颈部淋巴结转移肿瘤达到(n=43)与未达到客观缓解患者(n=15)的5年OS率分别为78.89%、80.00%,差异均无统计学意义(χ 2=0.239,P=0.625;χ 2=0.005,P=0.943);在T3-4期患者中,诱导化疗后鼻咽原发肿瘤达到(n=54)与未达到客观缓解患者(n=49)的5年OS率分别为78.90%、45.00%,颈部淋巴结转移肿瘤达到(n=61)与未达到客观缓解患者(n=42)的5年OS率分别为75.10%、42.89%,差异均有统计学意义(χ 2=13.615,P<0.001;χ 2=12.752,P<0.001)。单因素Cox回归分析表明,在T1-2期患者中,诱导化疗后肿瘤退缩率、鼻咽原发肿瘤及颈部淋巴结转移肿瘤疗效均与OS无关(均P>0.05);在T3-4期患者中,诱导化疗后鼻咽原发肿瘤退缩率(HR=0.121,95%CI为0.033~0.444,P=0.001)、颈部淋巴结转移肿瘤退缩率(HR=0.126,95%CI为0.036~0.442,P=0.001)、鼻咽原发肿瘤疗效(HR=0.297,95%CI为0.150~0.588,P<0.001)和颈部淋巴结转移肿瘤疗效(HR=0.329,95%CI为0.173~0.625,P=0.001)均与OS相关;多因素Cox回归分析发现,鼻咽原发肿瘤疗效与T分期交互项接近统计学意义(P=0.062)。结论 Ⅲ~ⅣA期鼻咽癌患者中,T3-4期患者诱导化疗后鼻咽部原发病灶缓解情况对预测生存预后具有重要价值。