Journal of International Oncology ›› 2020, Vol. 47 ›› Issue (11): 675-681.doi: 10.3760/cma.j.cn371439-20191224-00099
• Original Articles • Previous Articles Next Articles
Value of P16/Ki-67 double staining detection in screening cervical cancer and precancerous lesions
Song Mingze1, Cheng Yiming1, Li Gang2, Wang Zhenming2, Li Shirong2( )
)
- 1Department of Laboratory Medicine, Weifang Medical College, Weifang 261000, China
2Department of Laboratory Medicine, Weifang People's Hospital of Shandong Province, Weifang 261000, China
-
Received:2019-12-24Revised:2020-09-28Online:2020-11-08Published:2021-01-05 -
Contact:Li Shirong E-mail:lsr2270@163.com -
Supported by:Health and Family Planning Commission Scientific Research Project of Weifang of China(2017wsjs103)
Cite this article
Song Mingze, Cheng Yiming, Li Gang, Wang Zhenming, Li Shirong. Value of P16/Ki-67 double staining detection in screening cervical cancer and precancerous lesions[J]. Journal of International Oncology, 2020, 47(11): 675-681.
share this article

"
"
| 组别 | HPV DNA | TCT | P16/Ki-67 | |||||
|---|---|---|---|---|---|---|---|---|
| 阴性 | 阳性 | 阴性 | 阳性 | 阴性 | 阳性 | |||
| <CIN2组(n=110) | 89 | 21 | 83 | 27 | 90 | 20 | ||
| CIN2组(n=31) | 3 | 28 | 5 | 26 | 1 | 30 | ||
| CIN3组(n=27) | 2 | 25 | 1 | 26 | 1 | 26 | ||
| 宫颈癌组(n=12) | 1 | 11 | 3 | 9 | 0 | 12 | ||
"
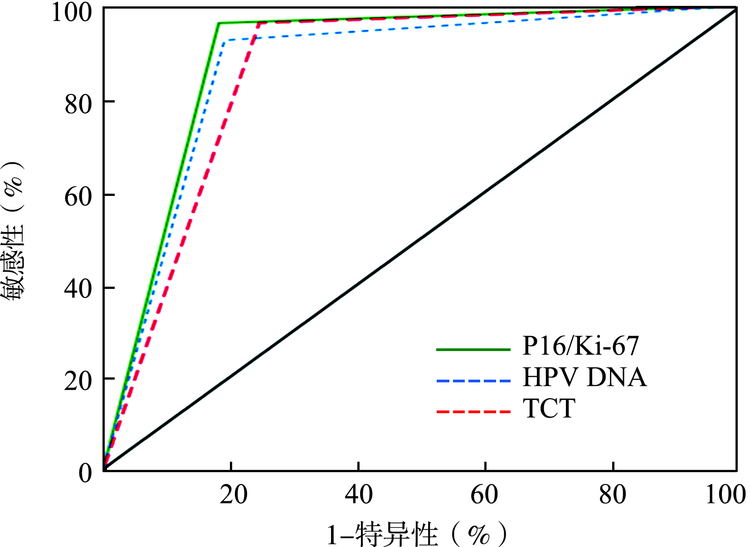
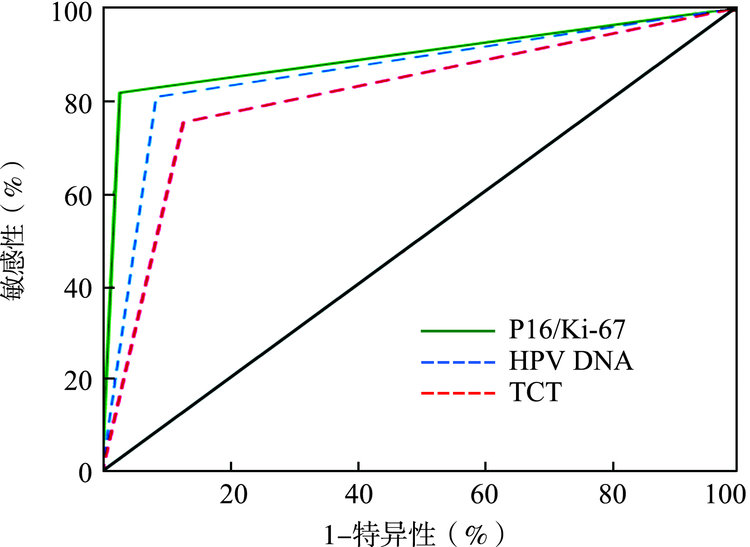
| 检测方法 | AUC值 | 敏感性(%) | 特异性(%) | 阳性预测值(%) | 阴性预测值(%) | Kappa值 |
|---|---|---|---|---|---|---|
| HPV DNA | 0.862 | 80.91 | 91.43a | 93.68 | 75.29 | 0.696 |
| TCT | 0.813 | 75.45a | 87.14a | 90.22a | 69.32 | 0.598 |
| P16/Ki-67 | 0.895 | 81.82 | 97.14 | 97.83 | 77.27 | 0.754 |
| χ2值 | 1.593 | 4.736 | 4.667 | 1.564 | ||
| P值 | 0.042 | 0.034 | 0.037 | 0.048 |
"
| 检测方法 | AUC值 | 敏感性(%) | 特异性(%) | 阳性预测值(%) | 阴性预测值(%) | Kappa值 |
|---|---|---|---|---|---|---|
| HPV DNA | 0.856 | 90.32b | 80.91 | 57.10 | 96.70 | 0.589 |
| TCT | 0.797 | 83.87a | 75.45 | 49.10 | 94.30a | 0.473 |
| P16/Ki-67 | 0.893 | 96.77 | 81.82 | 60.00 | 98.90 | 0.644 |
| χ2值 | 2.952 | 2.505 | 1.939 | 3.175 | ||
| P值 | 0.029 | 0.066 | 0.079 | 0.013 |
"
| 检测方法 | AUC值 | 敏感性(%) | 特异性(%) | 阳性预测值(%) | 阴性预测值(%) | Kappa值 |
|---|---|---|---|---|---|---|
| HPV DNA | 0.868 | 92.59 | 80.91 | 54.30 | 97.80 | 0.581 |
| TCT | 0.859 | 96.30 | 75.45a | 49.10a | 98.80 | 0.526 |
| P16/Ki-67 | 0.891 | 96.30 | 81.82 | 56.50 | 98.90 | 0.617 |
| χ2值 | 0.497 | 4.677 | 1.760 | 0.441 | ||
| P值 | 0.780 | 0.036 | 0.045 | 0.802 |
"
| 检测方法 | AUC值 | 敏感性(%) | 特异性(%) | 阳性预测值(%) | 阴性预测值(%) | Kappa值 |
|---|---|---|---|---|---|---|
| HPV DNA | 0.863 | 91.67 | 80.91 | 34.40 | 98.90 | 0.417 |
| TCT | 0.752 | 75.00a | 75.45 | 25.00 | 96.50 | 0.267 |
| P16/Ki-67 | 0.909 | 100.00 | 81.82 | 37.50 | 100.00 | 0.470 |
| χ2值 | 3.293 | 2.736 | 1.834 | 3.075 | ||
| P值 | 0.034 | 0.255 | 0.400 | 0.081 |
"
"
"
"
"
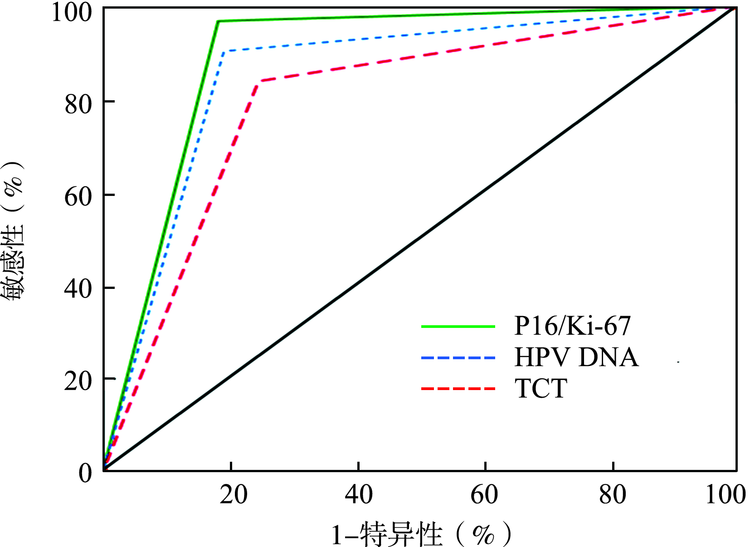
| 诊断指标 | ≥CIN2级(n=70) | χ2值 | P值 | ≥CIN3级(n=39) | χ2值 | P值 | ||
|---|---|---|---|---|---|---|---|---|
| TCT | P16/Ki-67 | TCT | P16/Ki-67 | |||||
| 敏感性 | 87.14 | 97.14 | 4.834 | 0.028 | 89.74 | 97.44 | 0.855 | 0.355 |
| 特异性 | 75.45 | 81.82 | 1.326 | 0.250 | 62.41 | 64.54 | 2.811 | 0.094 |
| 阳性预测值 | 69.32 | 77.27 | 1.422 | 0.233 | 39.77 | 43.18 | 1.906 | 0.167 |
| 阴性预测值 | 90.22 | 97.83 | 4.738 | 0.031 | 95.65 | 98.91 | 0.964 | 0.326 |
| 假阴性率 | 12.86 | 2.86 | 4.834 | 0.028 | 10.26 | 2.56 | 0.855 | 0.355 |
| 假阳性率 | 24.55 | 18.18 | 1.326 | 0.250 | 37.59 | 35.46 | 2.811 | 0.094 |
"
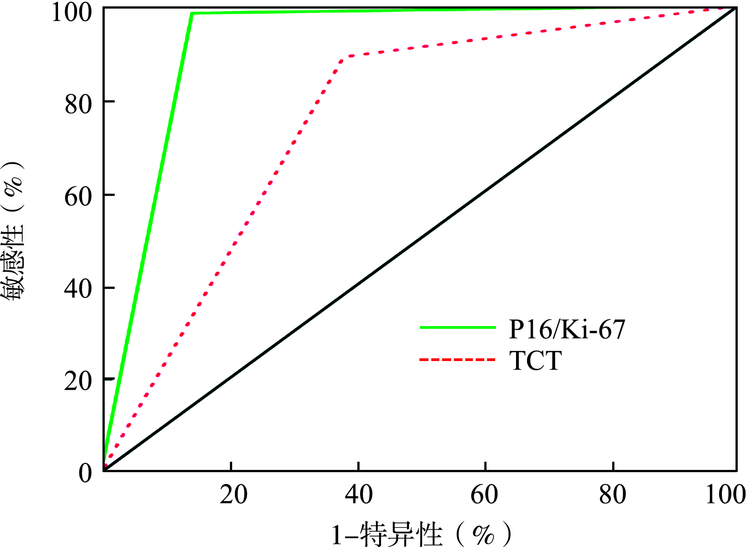
| 检测方法 | AUC值 | 敏感性 (%) | 特异性 (%) | 阳性预测值 (%) | 阴性预测值 (%) |
|---|---|---|---|---|---|
| TCT | 0.755 | 89.06 | 61.90 | 87.70 | 65.00 |
| P16/Ki-67 | 0.921 | 98.44 | 85.71 | 95.50 | 94.70 |
| χ2值 | 4.800 | 3.079 | 2.565 | 5.284 | |
| P值 | 0.028 | 0.039 | 0.109 | 0.022 |
"
| [1] | 王麟华, 吴玉梅, 于新平. DNA损伤修复在宫颈癌放疗敏感性中的研究进展[J]. 解放军预防医学杂志, 2019,37(8):193-194. |
| [2] | 周焕娣, 黄小军, 夏燕卿, 等. 探讨P16/Ki67蛋白检测在宫颈上皮内瘤变诊断中的应用[J]. 中国实用医药, 2018,13(12):16-17. DOI: 10.14163/j.cnki.11-5547/r.2018.12.007. |
| [3] | 颜丽, 周德平, 杨君. 人乳头瘤病毒L1壳蛋白在宫颈脱落细胞中的表达及其临床意义[J]. 重庆医科大学学报, 2016,41(10):1064-1068. DOI: 10.13406/j.cnki.cyxb.001031. |
| [4] | 李博涵, 谭桂春. 高危型人乳头瘤病毒阳性患者宫颈病变风险预测方法及进展[J]. 国际妇产科学杂志, 2019,46(1):98-103. DOI: 10.3969/j.issn.1674-1870.2019.01.025. |
| [5] | 王琳倩, 余辉, 高亮, 等. 液基细胞学联合DNA定量细胞学在筛查宫颈病变中的应用价值[J]. 中国优生与遗传杂志, 2014,22(5):14-17, 80. |
| [6] | 叶延青. HPV检测在宫颈未明确诊断意义的不典型鳞状上皮细胞中临床意义[J]. 中国实用医药, 2010,5(19):61-62. DOI: 10.3969/j.issn.1673-7555.2010.19.038. |
| [7] |
Liu G, Sharma M, Tan N, et al. HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer[J]. AIDS, 2018,32(6):795-808. DOI: 10.1097/QAD.0000000000001765.
doi: 10.1097/QAD.0000000000001765 pmid: 29369827 |
| [8] |
Arbyn M, Ronco G, Anttila A, et al. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer[J]. Vaccine, 2012,30 Suppl 5: F88-F99. DOI: 10.1016/j.vaccine.2012.06.095.
doi: 10.1016/j.vaccine.2012.06.095 |
| [9] |
Stanczuk GA, Baxter GJ, Currie H, et al. Defining optimal triage strategies for hrHPV screen-positive women-an evaluation of HPV 16/18 genotyping, cytology, and p16/Ki-67 cytoimmunochemistry[J]. Cancer Epidemiol Biomarkers Prev, 2017,26(11):1629-1635. DOI: 10.1158/1055-9965.EPI-17-0534.
doi: 10.1158/1055-9965.EPI-17-0534 pmid: 28887297 |
| [10] |
Wentzensen N, Schiffman M, Palmer T, et al. Triage of HPV positive women in cervical cancer screening[J]. J Clin Virol, 2016,76 Suppl 1: S49-S55. DOI: 10.1016/j.jcv.2015.11.015.
doi: 10.1016/j.jcv.2015.11.015 |
| [11] |
Rijkaart DC, Berkhof J, van Kemenade FJ, et al. Evaluation of 14 triage strategies for HPV DNA-positive women in population-based cervical screening[J]. Int J Cancer, 2012,130(3):602-610. DOI: 10.1002/ijc.26056.
doi: 10.1002/ijc.26056 pmid: 21400507 |
| [12] |
Wentzensen N, von Knebel Doeberitz M. Biomarkers in cervical cancer screening[J]. Dis Markers, 2007,23(4):315-30. DOI: 10.1155/2007/678793.
doi: 10.1155/2007/678793 pmid: 17627065 |
| [13] |
da Costa LBE, Triglia RM, Andrade L. p16INK4a, cytokeratin 7, and Ki-67 as potential markers for low-grade cervical intraepithelial neoplasia progression[J]. J Low Genit Tract Dis, 2017,21(3):171-176. DOI: 10.1097/LGT.0000000000000310.
doi: 10.1097/LGT.0000000000000310 pmid: 28403025 |
| [14] |
Ciavattini A, Sopracordevole F, Di Giuseppe J, et al. Cervical intraepithelial neoplasia in pregnancy: interference of pregnancy status with p16 and Ki-67 protein expression[J]. Oncol Lett, 2017,13(1):301-306. DOI: 10.3892/ol.2016.5441.
doi: 10.3892/ol.2016.5441 pmid: 28123559 |
| [15] |
Uijterwaal MH, Polman NJ, Witte BI, et al. Triaging HPV-positive women with normal cytology by p16/Ki-67 dual-stained cytology testing: baseline and longitudinal data[J]. Int J Cancer, 2015,136(10):2361-2368. DOI: 10.1002/ijc.29290.
doi: 10.1002/ijc.29290 pmid: 25345358 |
| [16] | 梁江红, 罗蕊丽. p16/Ki67细胞学双染检测对宫颈癌筛查患者的分流管理现状[J]. 湖北医药学院学报, 2016,35(2):228-230. DOI: 10.13819/j.issn.1006-9674.2016.02.029. |
| [17] |
Celewicz A, Celewicz M, Wezowska M, et al. Clinical efficacy of p16/Ki-67 dual-stained cervical cytology in secondary prevention of cervical cancer [J]. Pol J Pathol, 2018,69(1):42-47. DOI: 10.5114/pjp.2018.75335.
doi: 10.5114/pjp.2018.75335 pmid: 29895125 |
| [18] |
Zhang R, Ge X, You K, et al. p16/Ki67 dual staining improves the detection specificity of high-grade cervical lesions[J]. J Obstet Gynaecol Res, 2018,44(11):2077-2084. DOI: 10.1111/jog.13760.
doi: 10.1111/jog.13760 pmid: 30094887 |
| [19] |
Areán-Cuns C, Mercado-Gutiérrez M, Paniello-Alastruey I, et al. Dual staining for p16/Ki67 is a more specific test than cytology for triage of HPV-positive women[J]. Virchows Arch, 2018,473(5):599-606. DOI: 10.1007/s00428-018-2432-z.
doi: 10.1007/s00428-018-2432-z pmid: 30094492 |
| [1] | Guo Zehao, Zhang Junwang. Role of PFDN and its subunits in tumorigenesis and tumor development [J]. Journal of International Oncology, 2024, 51(6): 350-353. |
| [2] | Zhang Ningning, Yang Zhe, Tan Limei, Li Zhenning, Wang Di, Wei Yongzhi. Diagnostic value of cervical cell DNA ploidy analysis combined with B7-H4 and PKCδ for cervical cancer [J]. Journal of International Oncology, 2024, 51(5): 286-291. |
| [3] | Liu Xiaodi, Su Jianfei, Zhang Jingxian, Wei Xueqin, Jia Yingjie. Research progress of myeloid-derived suppressor cells in tumor angiogenesis [J]. Journal of International Oncology, 2024, 51(1): 50-54. |
| [4] | Ye Tongtong, Wu Zeyu, Xi Wenyi, Wang Zhiwei, Jiang Xiaochun, Zhao Chenhui. Role of ABRACL in the occurrence and development of malignant tumors [J]. Journal of International Oncology, 2023, 50(9): 544-547. |
| [5] | Pan Shulan, Liu Chang, He Ping. Effect of fritinib on angiogenesis, tumor growth and IRE1-ASK1-JNK pathway in triple negative breast cancer [J]. Journal of International Oncology, 2023, 50(8): 457-462. |
| [6] | Zhang Lu, Jiang Hua, Lin Zhou, Ma Chenying, Xu Xiaoting, Wang Lili, Zhou Juying. Analysis of curative effect and prognosis of immune checkpoint inhibitor in the treatment of recurrent and metastatic cervical cancer [J]. Journal of International Oncology, 2023, 50(8): 475-483. |
| [7] | Zhang Yuan, Bai Zhiyu, Li Qi, Feng Qinmei. Current status of research on exosomes in malignancies [J]. Journal of International Oncology, 2023, 50(8): 484-488. |
| [8] | Lyu Lu, Sun Pengfei. Gut flora and cervical cancer [J]. Journal of International Oncology, 2023, 50(6): 373-376. |
| [9] | Liu Yujie, Zhao Zhiqiang, Wang Zicheng. Levels and diagnostic value of TOP2A and ERBB2 in peripheral blood mononuclear cells of patients with early colorectal cancer [J]. Journal of International Oncology, 2023, 50(12): 717-722. |
| [10] | Deng Lili, Duan Xingyu, Li Baozhong. Advances of anti-HER2 targeted drugs and combined therapeutic regimens for gastric and esophagogastic adenocarcinoma [J]. Journal of International Oncology, 2023, 50(12): 751-757. |
| [11] | Ma Xueyan, Lu Lili, Sun Pengfei. Advances in the immune microenvironment in cervical cancer [J]. Journal of International Oncology, 2023, 50(1): 47-50. |
| [12] | Zhang Lu, Zhou Juying, Ma Chenying, Lin Zhou. Advances in immunotherapy for recurrent and metastatic cervical cancer [J]. Journal of International Oncology, 2022, 49(9): 517-520. |
| [13] | Shi Yingxia, Hu Lijun, Yu Jingping. Application of immune checkpoint inhibitors in the treatment of recurrent or metastatic cervical cancer [J]. Journal of International Oncology, 2022, 49(9): 568-571. |
| [14] | Peng Chen, Xie Yintong, Zhang Xin, Xie Peng. Research progress of maintenance therapy for cervical cancer [J]. Journal of International Oncology, 2022, 49(7): 430-435. |
| [15] | Yuan Chenyang, Zhou Juying. Research progress on prognostic factors of cervical cancer [J]. Journal of International Oncology, 2022, 49(5): 307-313. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||