国际肿瘤学杂志 ›› 2021, Vol. 48 ›› Issue (9): 515-522.doi: 10.3760/cma.j.cn371439-20201214-00100
陈方明1, 蔡园园2, 李晗3, 王晓丽2, 阚红星4, 李洋2, 郝福荣2( ), 王明臣2()
), 王明臣2()
Chen Fangming1, Cai Yuanyuan2, Li Han3, Wang Xiaoli2, Kan Hongxing4, Li Yang2, Hao Furong2(), Wang Mingchen2()
摘要:
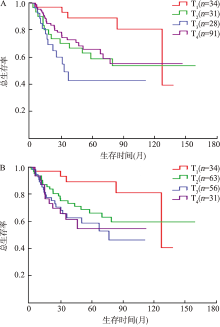
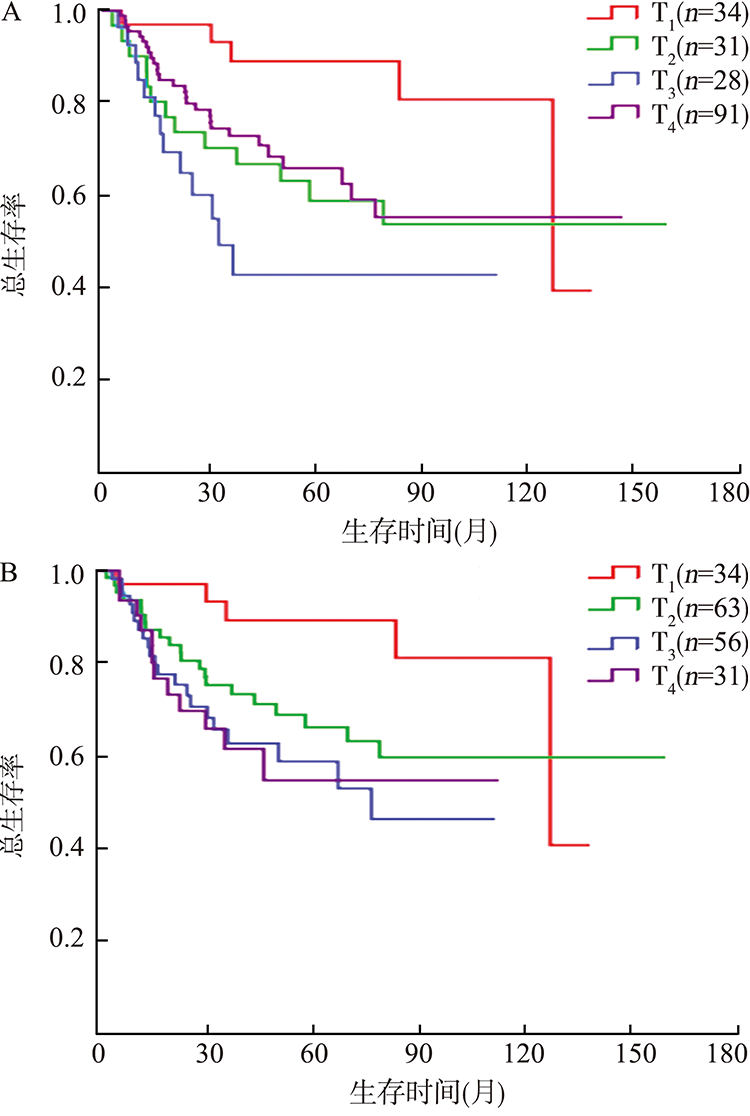
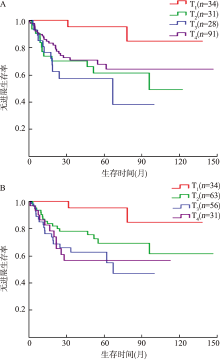
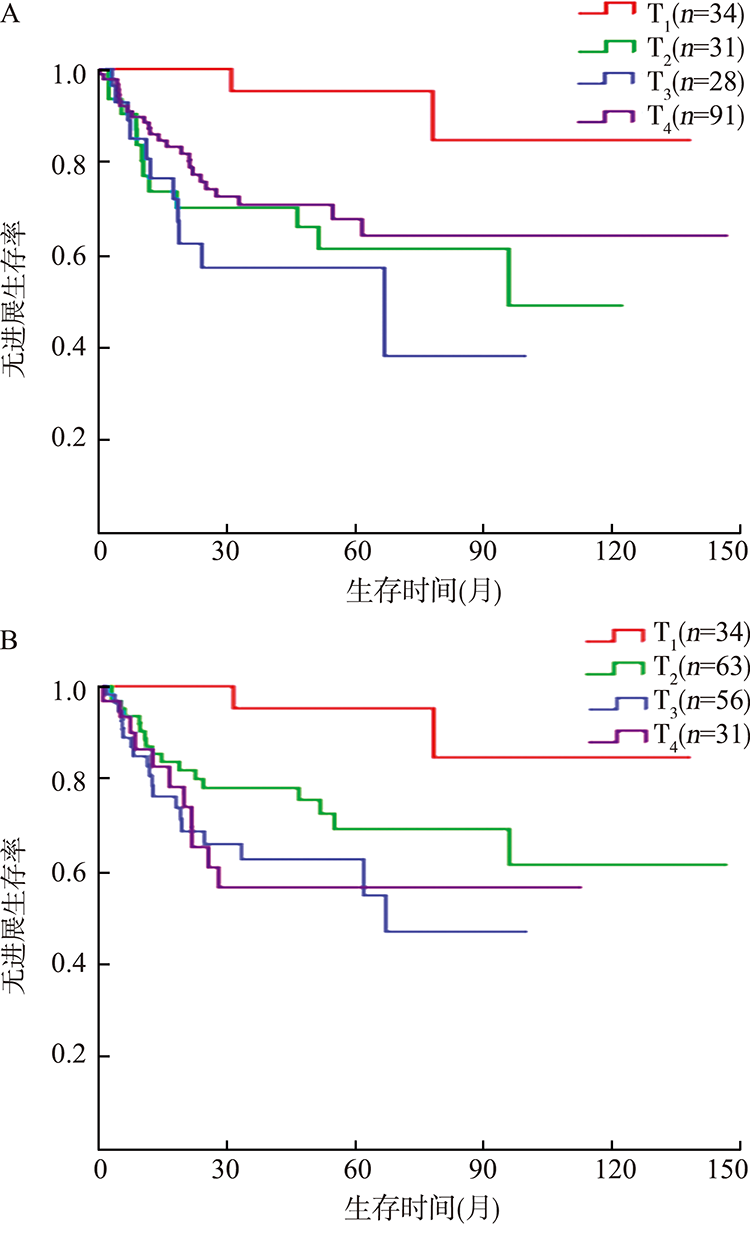
目的 比较调强放疗鼻咽癌在国际抗癌联盟(UICC)鼻咽癌第7版(简称UICC 7版)与第8版(简称UICC 8版)T分期的人群分布和预后差异,并分析鼻咽癌患者的预后影响因素。方法 回顾性分析2005年6月1日至2017年12月31日山东省潍坊市人民医院放疗科收治的184例初治调强放疗鼻咽癌患者的临床病理资料,按UICC 7版、UICC 8版对入组病例进行重新分期,分析两版分期系统患者T分期的分布,采用Kappa一致性检验比较两种分期的一致性。采用Kaplan-Meier法进行生存分析,log-rank检验比较各T分期之间的预后差异。采用Cox回归模型分析鼻咽癌患者的预后影响因素。结果 184例调强放疗鼻咽癌患者按UICC 7版T分期,T1、T2、T3和T4期分别占18.5%(34/184)、16.8%(31/184)、15.2%(28/184)、49.5%(91/184),而按UICC 8版T分期,分别占18.5%(34/184)、34.2%(63/184)、30.4%(56/184)和16.8%(31/184),两版分期系统的T分期人群分布具有中度一致性(Kappa=0.58)。UICC 7版分期中,T1、T2、T3、T4期患者的总生存期(OS)差异有统计学意义(χ2=10.606,P=0.014),T1与T2、T3、T4期患者的OS差异均有统计学意义(χ2=4.866,P=0.027;χ2=11.965,P=0.001;χ2=4.351,P=0.037),T2、T4期OS曲线不能分离,T3、T4期OS曲线倒序分布;UICC 8版分期中,4期患者的OS差异有统计学意义(χ2=8.663,P=0.034),T1与T3、T4期患者的OS差异均有统计学意义(χ2=8.746,P=0.003;χ2=7.580,P=0.006),T1~T4期的OS曲线顺序分布,T3与T4期OS曲线仍未能分离。UICC 7版分期中,T1、T2、T3、T4期患者的无进展生存期(PFS)差异有统计学意义(χ2=11.289,P=0.010),T1与T2、T3、T4期患者的PFS差异均有统计学意义(χ2=8.209,P=0.004;χ2=13.302,P<0.001;χ2=6.550,P=0.010),T2、T4期PFS曲线不能分离,T3、T4期PFS曲线倒序分布;UICC 8版分期中,4期患者的PFS差异有统计学意义(χ2=12.074,P=0.007),T1与T2、T3、T4期患者的PFS差异均有统计学意义(χ2=5.182,P=0.023;χ2=11.217,P=0.001;χ2=10.174,P=0.001),T1~T4期的PFS曲线顺序分布,但T3与T4期PFS曲线未能分离。分别按UICC 7版和8版分期行Cox多因素分析,结果显示两版分期中T分期均是患者OS(P=0.013;P=0.026)、PFS(P=0.031;P=0.012)的独立预后因素,但两版分期中T分期均不是患者无局部复发生存期(LRFS)(P=0.351;P=0.167)、无远处转移生存期(DMFS)(P=0.059;P=0.052)的独立预后因素;两版分期中年龄均是影响OS(HR=2.70,95%CI为1.53~4.76,P=0.001;HR=2.74,95%CI为1.55~4.84,P=0.001)、PFS(HR=2.72,95%CI为1.46~5.08,P=0.002;HR=2.94,95%CI为1.57~5.52,P=0.001)、LRFS(HR=5.87,95%CI为1.62~21.27,P=0.007;HR=6.02,95%CI为1.61~22.49,P=0.008)及DMFS(HR=2.40,95%CI为1.22~4.72,P=0.011;HR=2.63,95%CI为1.34~5.18,P=0.005)的独立预后因素,N分期是影响OS(P=0.031;P=0.028)的独立预后因素。结论 UICC 7版与8版分期系统的T分期人群分布具有中等一致性,UICC 8版T分期对OS及PFS的预后判断更有优势,两版分期中T分期均是患者OS、PFS的独立预后因素。