国际肿瘤学杂志 ›› 2020, Vol. 47 ›› Issue (2): 77-81.doi: 10.3760/cma.j.issn.1673-422X.2020.02.003
马超1,2, 蔡洪庆2, 张敏杰1,2, 叶士露1,2, 孟肖利2, 何洁1, 万经海1,2( )
)
Ma Chao1,2, Cai Hongqing2, Zhang Minjie1,2, Ye Shilu1,2, Meng Xiaoli2, He Jie1, Wan Jinghai1,2()
摘要:
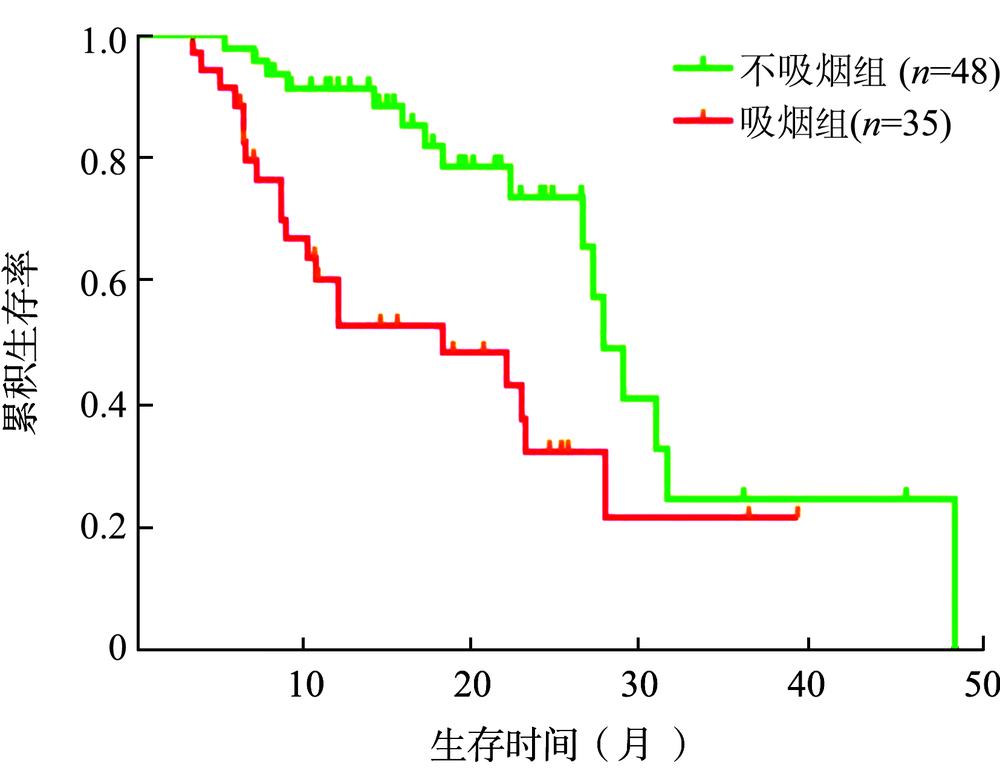
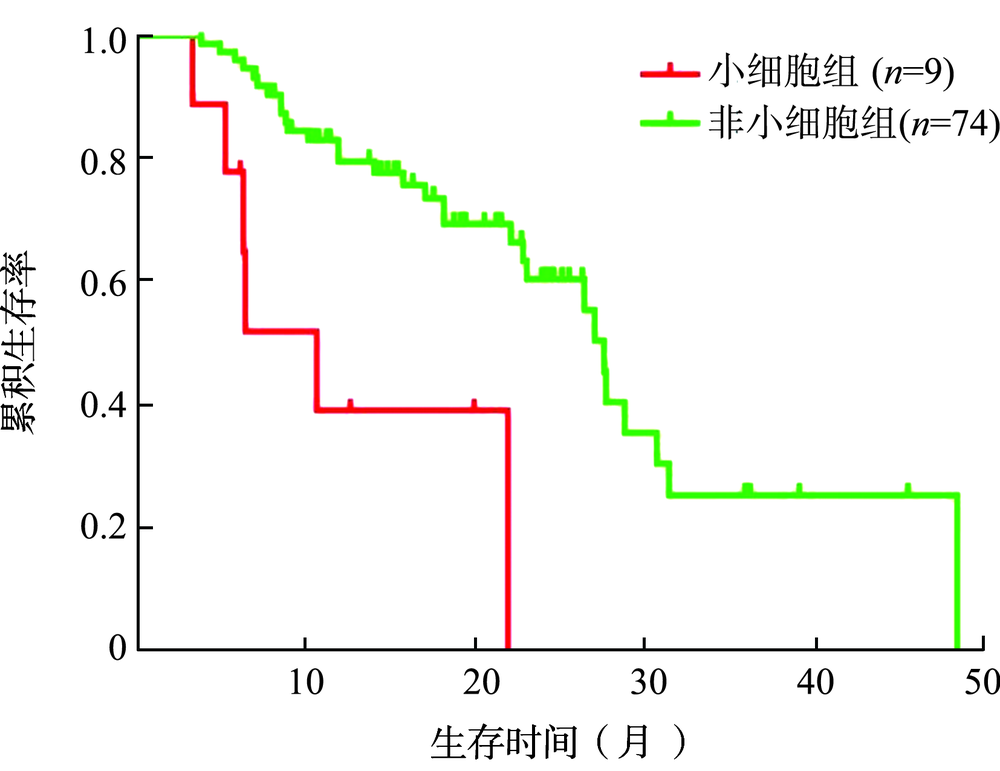
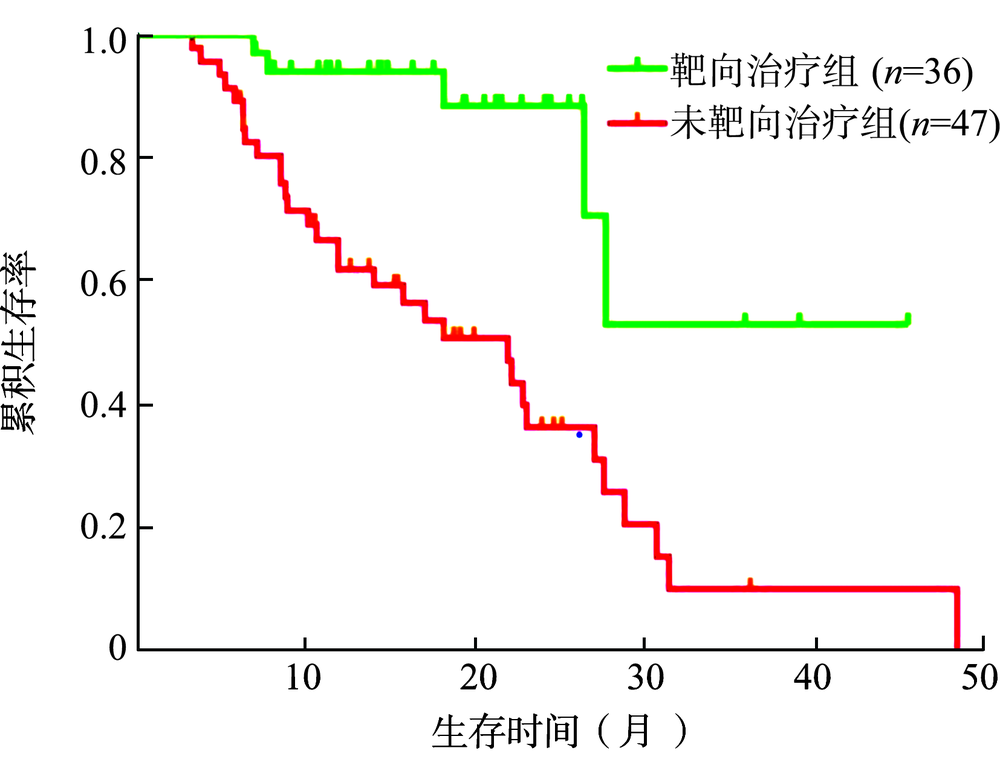
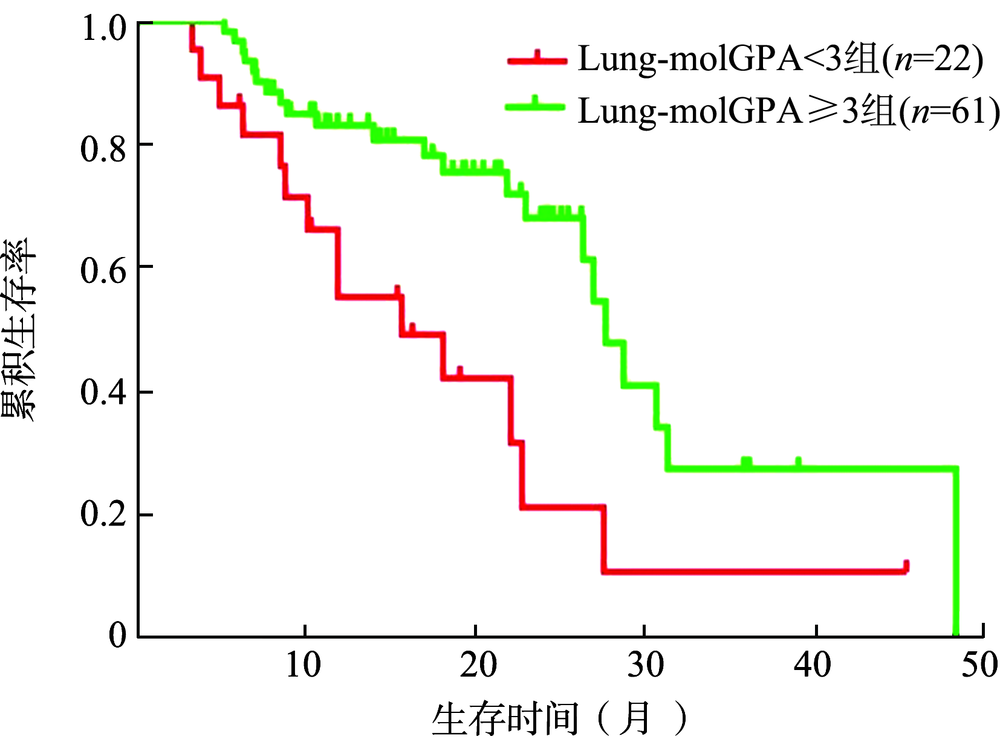
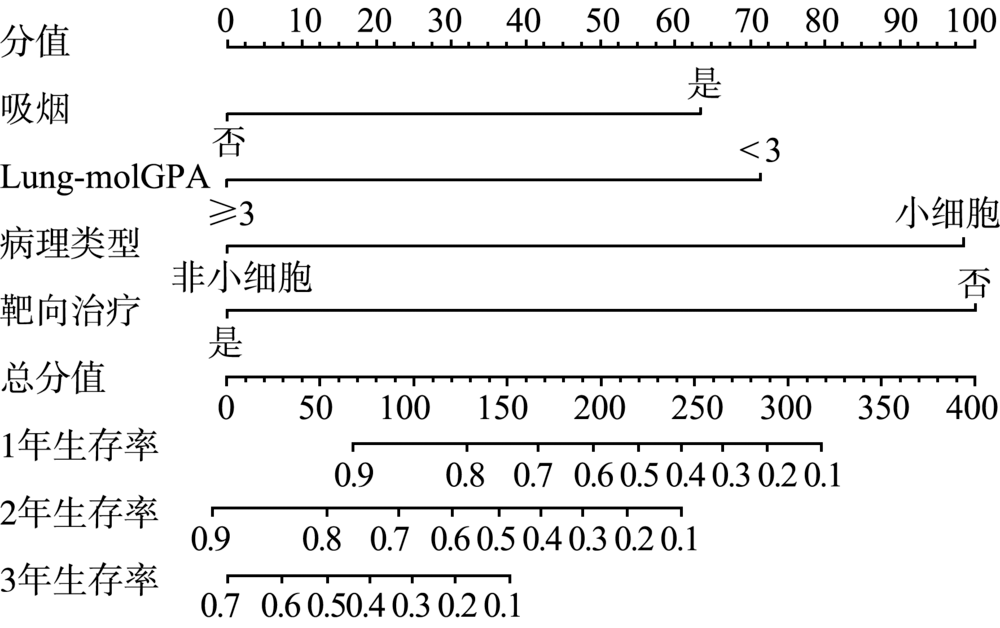
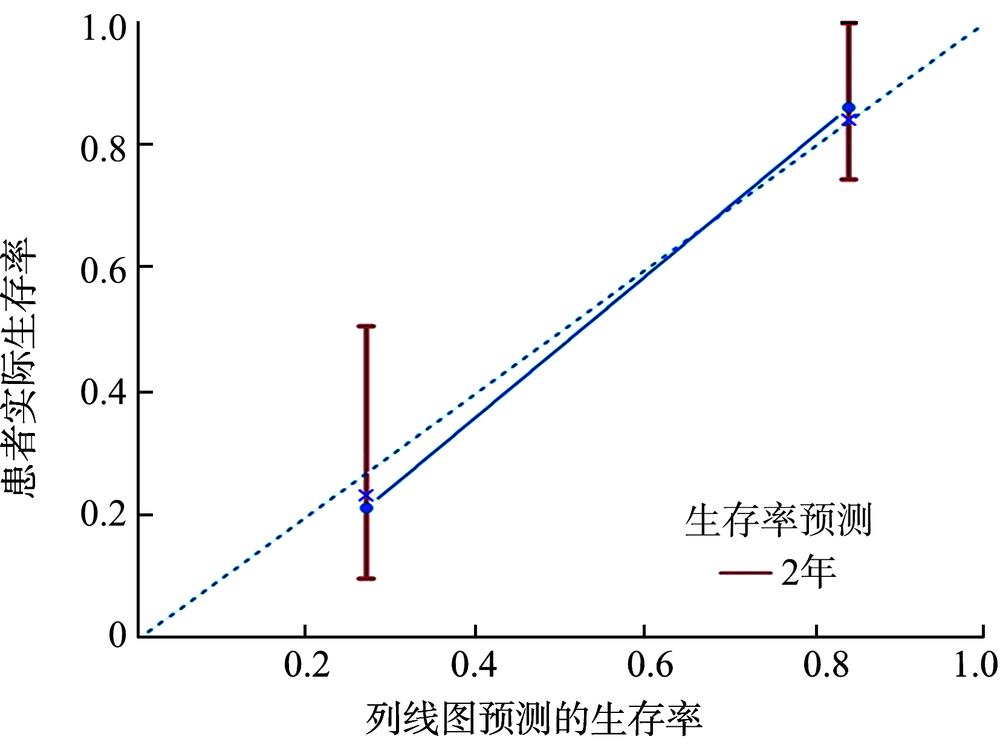
目的 对肺癌脑转移行手术治疗的患者进行预后相关因素分析。方法 回顾性收集2016年1月至2018年11月在中国医学科学院北京协和医学院肿瘤医院神经外科行手术治疗的肺癌脑转移患者的临床资料,获得完整的资料共83例,单因素分析采用log-rank法,多因素分析采用Cox风险比例模型,应用R软件将影响因素绘制成列线图并进行验证。结果 83例患者的中位总生存期(OS)为27.0个月。单纯手术患者中位OS为15.7个月,手术联合放疗、化疗或靶向治疗患者的中位OS为27.7个月,差异有统计学意义(χ 2=8.735,P=0.003)。单因素分析结果显示,性别(χ 2=4.652,P=0.031)、有无吸烟史(χ 2=8.239,P=0.004)、术后是否靶向治疗(χ 2=13.697,P<0.001)、术后有无辅助治疗(χ 2=8.735,P=0.003)、转移灶病理(χ 2=11.799,P=0.001)、肺肿瘤相关分子分级预后评估指数(Lung-molGPA)评分(χ 2=11.333,P=0.004)可影响患者OS。多因素分析结果显示,吸烟史(HR=0.311,95%CI为0.107~0.901,P=0.031)、术后靶向治疗(HR=3.563,95%CI为1.286~9.868,P=0.015)、转移灶病理(HR=0.364,95%CI为0.137~0.965,P=0.042)、Lung-molGPA评分(HR=0.595,95%CI为0.374~0.946,P=0.028)是影响肺癌脑转移手术患者OS的独立预后因素。为了进一步个体化评估患者预后,采用以上4个独立的预后因素绘制了列线图,该模型准确度较高,能较好地评估患者的预后生存情况。结论 有手术指征的肺癌脑转移患者能从手术中受益,术后积极辅助治疗可进一步延长患者OS。采用吸烟、靶向治疗、转移灶病理、Lung-molGPA评分4个因素构建的列线图可以很好地个体化评估患者预后并指导临床治疗。