国际肿瘤学杂志 ›› 2022, Vol. 49 ›› Issue (3): 151-163.doi: 10.3760/cma.j.cn371439-20211015-00026
袁晨阳, 周菊英( ), 杜霄, 纪环, 赵天翼
), 杜霄, 纪环, 赵天翼
Yuan Chenyang, Zhou Juying(), Du Xiao, Ji Huan, Zhao Tianyi
摘要:
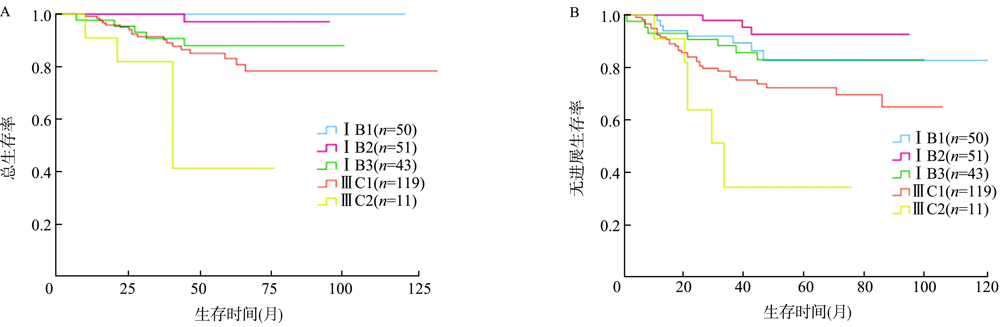
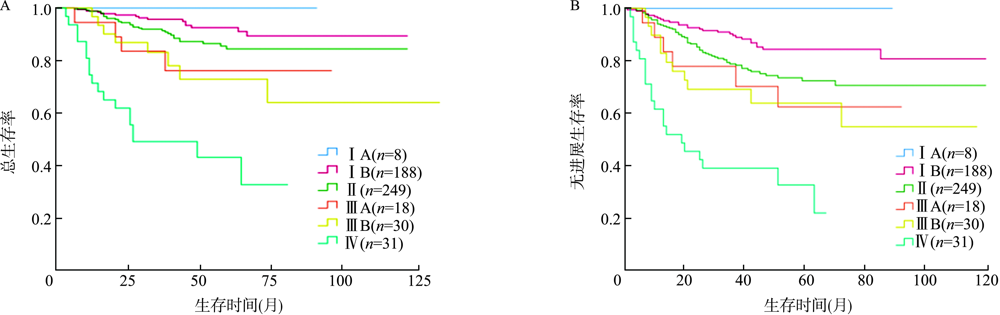
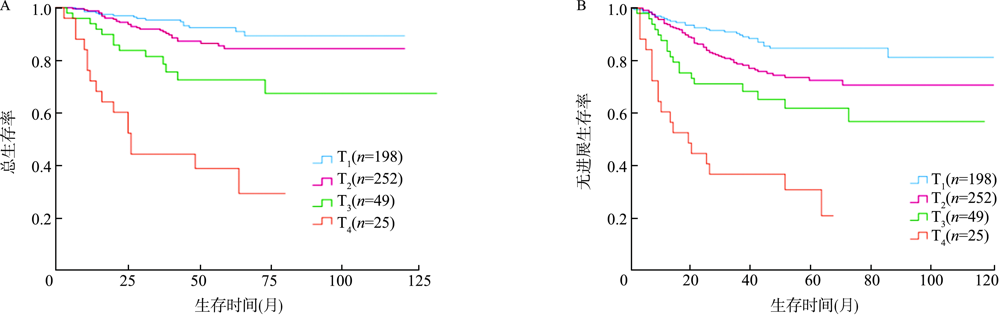
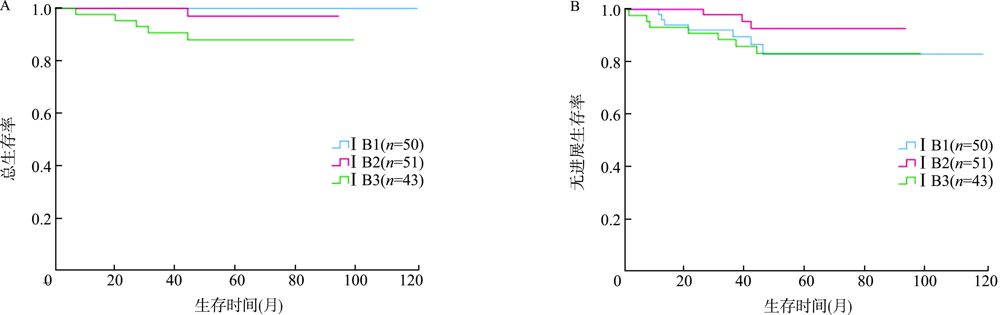
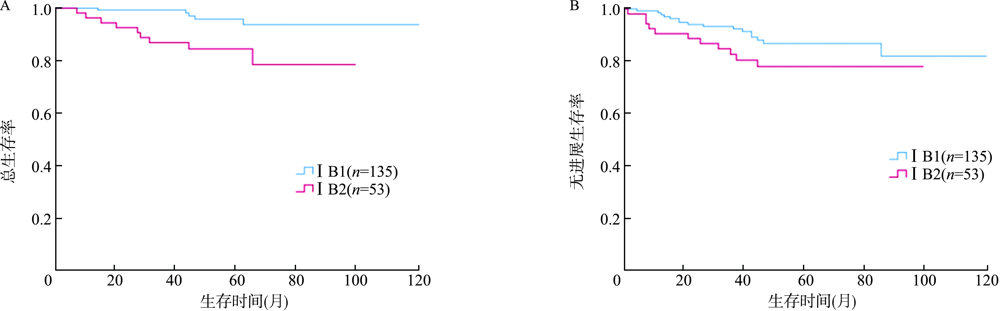
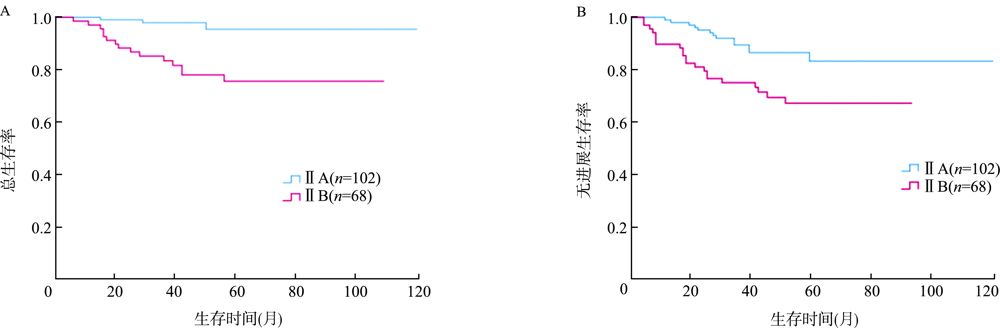
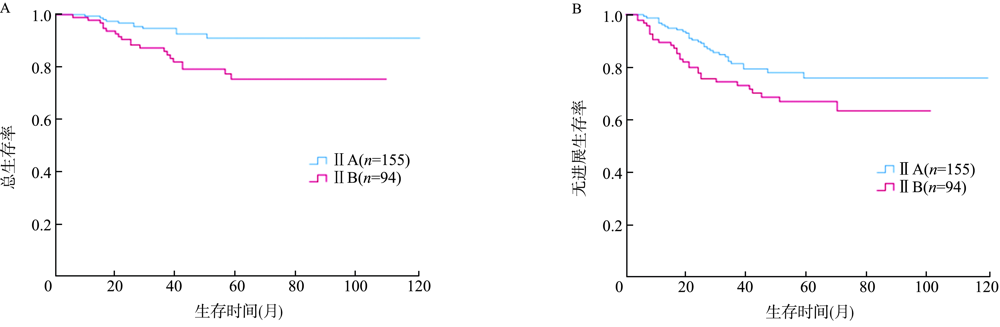
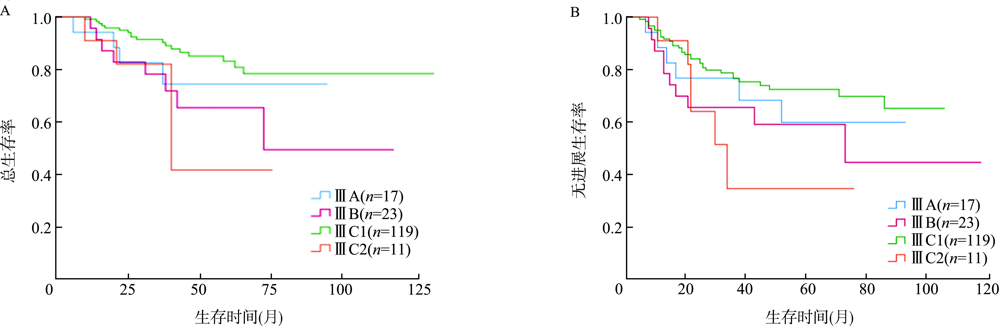
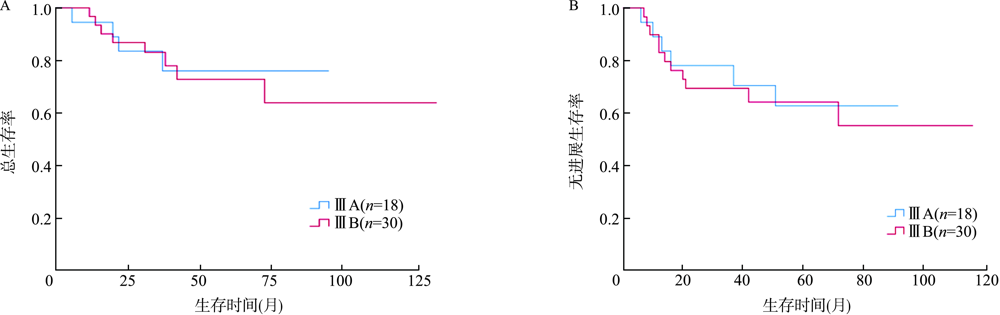
目的 比较宫颈癌患者在2009和2018两版国际妇产科联盟(FIGO)分期的分布和预后差异,并分析宫颈癌患者的预后因素。方法 回顾性分析2010年1月至2018年12月苏州大学附属第一医院收治的524例宫颈癌患者的临床资料,按照2009和2018 FIGO分期分别对病例进行分期,计算Kendall τb系数比较两种分期病例分布的一致性;采用Kaplan-Meier法进行生存分析,log-rank检验各期预后差异。采用Cox比例风险回归模型分析宫颈癌患者的预后因素。结果 2009 FIGO分期中有1例ⅠB1期因镜下浸润深度<5 mm降至ⅠA1期,51例ⅠB1期因2 cm<肿瘤最大径≤4 cm上升至ⅠB2期,43例ⅠB2期因肿瘤最大径>4 cm上升至ⅠB3期,119例因盆腔淋巴结转移上升至ⅢC1期,11例因腹主动脉旁淋巴结转移上升至ⅢC2期。两种分期病例分布一致性较好(τb=0.61,P<0.001)。2018(ⅠA、ⅠB、Ⅱ、ⅢA、ⅢB、ⅢC1、ⅢC2、Ⅳ)、2009(ⅠA、ⅠB、Ⅱ、ⅢA、ⅢB、Ⅳ)FIGO各期患者以及不同T分期(T1、T2、T3、T4)患者的总生存期(OS)(χ 2=107.13,P<0.001;χ2=93.02,P<0.001;χ2=92.74,P<0.001)和无进展生存期(PFS)(χ2=91.95,P<0.001;χ2=77.69,P<0.001;χ2=73.27,P<0.001)差异均有统计学意义,其中2018 FIGOⅠB和ⅢC期的OS(χ2=20.71,P<0.001)与PFS(χ2=24.25,P<0.001)差异均有统计学意义,ⅢC1期和ⅠB2期的OS差异有统计学意义(χ2=6.18,P=0.013)。多因素分析结果显示,年龄(HR=1.88,95%CI为1.08~3.28,P=0.026)、病理类型(HR=2.11,95%CI为1.04~4.27,P=0.038)、淋巴结转移(HR=2.18,95%CI为1.34~3.56,P=0.002)、宫旁扩散(HR=2.56,95%CI为1.52~4.29,P<0.001)、肿瘤最大径(HR=1.98,95%CI为1.18~3.30,P=0.009)、治疗后鳞状细胞癌相关抗原(SCCA)阳性(HR=4.49,95%CI为2.09~9.68,P<0.001)、治疗前血红蛋白(HB)水平(HR=0.58,95%CI为0.35~0.96,P=0.035)均为影响宫颈癌患者OS的独立危险因素。按2018 FIGO分期,ⅠB1、ⅠB2、ⅠB3期患者5年OS率分别为100%、97.1%、87.9%,差异有统计学意义(χ2=7.79,P=0.020),ⅠB1和ⅠB3期差异有统计学意义(χ2=5.55,P=0.019);按2009 FIGO分期,ⅠB1、ⅠB2期患者5年OS率分别为95.7%、84.3%,差异有统计学意义(χ2=9.08,P=0.003)。对于2018 FIGOⅠB期患者,治疗后SCCA阳性(HR=1 172.50,95%CI为10.37~132 554.51,P=0.003)为影响OS的独立危险因素;分化程度(HR=0.09,95%CI为0.01~0.81,P=0.032)、治疗方式(HR=0.17,95%CI为0.04~0.71,P=0.015)、治疗后SCCA阳性(HR=190.68,95%CI为14.27~2 547.67,P<0.001)均为影响PFS的独立危险因素。对于2009 FIGOⅠB期患者,分期(HR=9.56,95%CI为2.38~38.32,P=0.001)、治疗后SCCA阳性(HR=126.32,95%CI为12.36~1 290.60,P<0.001)、淋巴结转移(HR=20.07,95%CI为3.63~111.11,P=0.001)均为影响OS的独立危险因素;分化程度(HR=0.11,95%CI为0.02~0.63,P=0.013)、治疗方式(HR=0.22,95%CI为0.06~0.75,P=0.015)、治疗后SCCA阳性(HR=43.83,95%CI为7.94~241.84,P<0.001)均为影响PFS的独立危险因素。按2018 FIGO分期,ⅡA、ⅡB期患者5年OS率分别为95.7%、75.6%,差异有统计学意义(χ2=13.96,P<0.001);ⅡA、ⅡB期患者5年PFS率分别为83.1%、67.1%,差异有统计学意义(χ2=7.61,P=0.006)。按2009 FIGO分期,ⅡA、ⅡB期患者5年OS率分别为90.9%、75.0%,差异有统计学意义(χ2=8.85,P=0.003);ⅡA、ⅡB期患者5年PFS率分别为75.7%、66.7%,差异有统计学意义(χ2=4.07,P=0.044)。对于2018 FIGOⅡ期患者,病理类型(HR=20.28,95%CI为2.93~140.32,P=0.002)、分期(HR=4.35,95%CI为1.02~18.55,P=0.047)均为影响OS的独立危险因素。对于2009 FIGOⅡ期患者,病理类型(HR=5.82,95%CI为1.62~20.94,P=0.007)为影响OS的独立危险因素;病理类型(HR=3.09,95%CI为1.22~7.85,P=0.017)、淋巴结转移(HR=2.07,95%CI为1.22~3.51,P=0.007)均为影响PFS的独立危险因素。对于2018 FIGOⅢ期患者,肿瘤最大径(HR=3.31,95%CI为1.45~7.56,P=0.005)、治疗后SCCA阳性(HR=4.67,95%CI为1.22~17.86,P=0.024)均为影响患者OS的独立危险因素;病理类型(HR=4.15,95%CI为1.47~11.77,P=0.007)、治疗后SCCA阳性(HR=3.96,95%CI为1.45~10.86,P=0.007)均为影响患者PFS的独立危险因素。结论 2018和2009 FIGO分期在宫颈癌患者中分布一致性较好,2018 FIGOⅠB期对预后的判断更具优势,但是ⅢC期并不能准确地判断预后,淋巴结转移情况和肿瘤最大径是较为重要的预后因素。