国际肿瘤学杂志 ›› 2025, Vol. 52 ›› Issue (9): 566-575.doi: 10.3760/cma.j.cn371439-20250417-00096
吴松友1,2, 王刚1,2,3( ), 王文玲1,2,3, 董洪敏1,2,3, 陈唯唯1,2,3, 李小凯1,2,3, 陈望花1,2,3, 左凯1,2,3
), 王文玲1,2,3, 董洪敏1,2,3, 陈唯唯1,2,3, 李小凯1,2,3, 陈望花1,2,3, 左凯1,2,3
Wu Songyou1,2, Wang Gang1,2,3(), Wang Wenling1,2,3, Dong Hongmin1,2,3, Chen Weiwei1,2,3, Li Xiaokai1,2,3, Chen Wanghua1,2,3, Zuo Kai1,2,3
摘要:
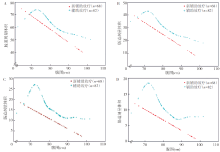
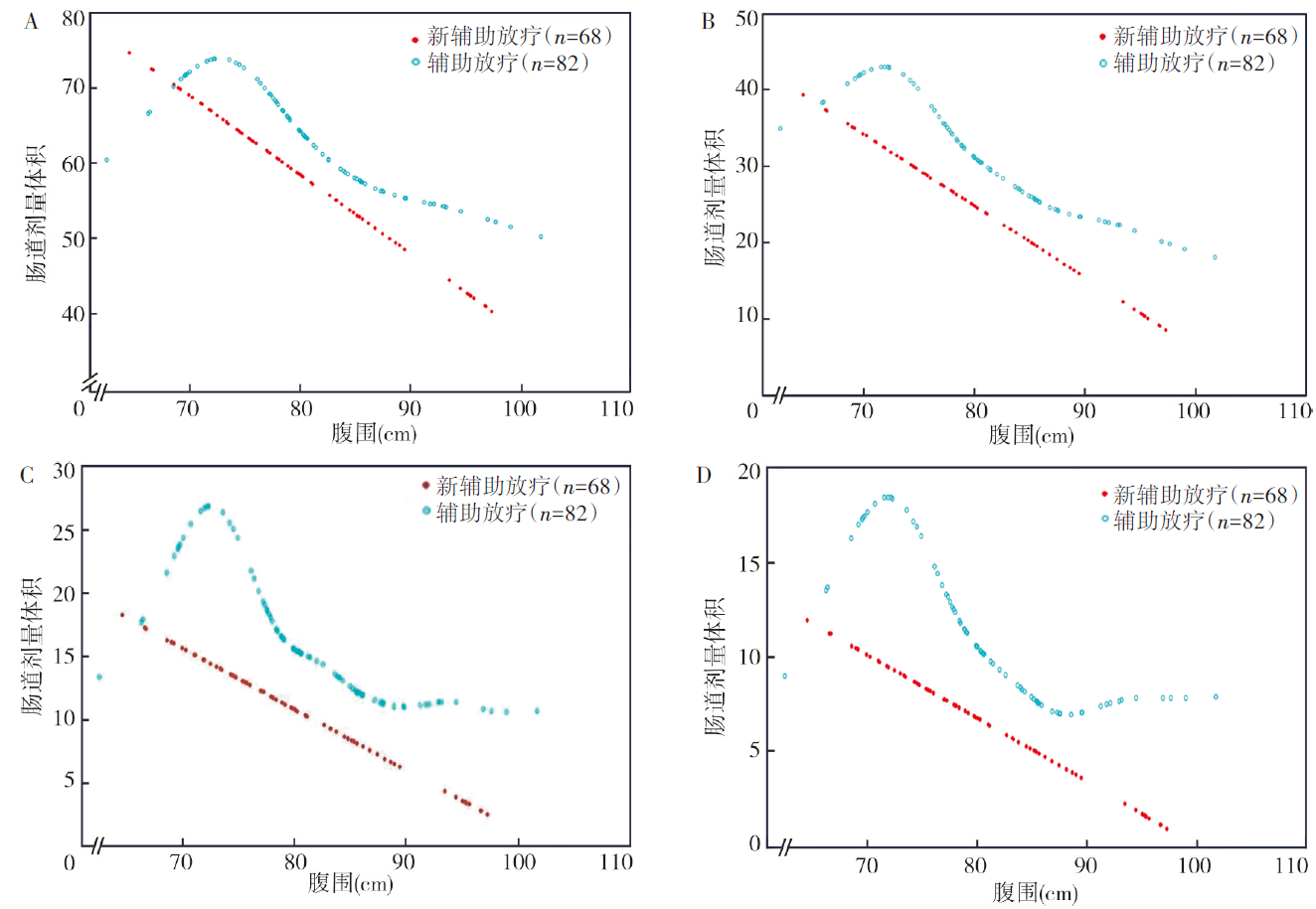
目的 探究直肠癌盆腔调强放疗中腹围对肠道受照剂量体积及急性肠道毒性的影响。方法 收集2023年3月至2025年1月在贵州医科大学附属肿瘤医院接受辅助和新辅助同步放化疗治疗的150例局部进展期直肠癌(LARC)患者,其中辅助放疗82例,新辅助放疗68例。所有患者均按俯卧位垫腹板并膀胱充盈的标准模式进行放疗CT模拟定位。根据是否发生≥2级急性肠道毒性将肠道毒性处理为二分类变量。采用线性及logistic回归模型分析LARC患者各个肠道受照剂量体积(V10、V20、V30、V40)、急性肠道毒性的影响因素,采用广义相加模型和分段线性及logistic回归分析腹围与肠道受照剂量体积和急性肠道毒性的阈值效应。根据阈值95%CI上限确定腹围界值,利用差异性检验验证小腹围和中大腹围在肠道受照剂量体积和急性肠道毒性的差异。结果 单因素分析显示,性别、体质量、腹围、计划靶区(PTV)、肠道体积均是辅助放疗LARC患者各个肠道受照剂量体积(V10、V20、V30、V40)的影响因素(均P<0.05),体质量、腹围、肠道体积均是新辅助放疗LARC患者各个肠道受照剂量体积(V10、V20、V30、V40)的影响因素(均P<0.05),体质量指数(BMI)、腹围、肠道体积、各个肠道受照体积(V10、V20、V30、V40)均是辅助放疗LARC患者急性肠道毒性的影响因素(均P<0.05),体质量、BMI、腹围、多个肠道受照剂量体积(V20、V30、V40)均是新辅助放疗LARC患者急性肠道毒性的影响因素(均P<0.05)。多因素分析显示,腹围(V10:β=-1.01,95%CI为-1.68~-0.33,P=0.004;V20:β=-0.94,95%CI为-1.28~-0.60,P<0.001;V30:β=-0.58,95%CI为-0.82~-0.34,P<0.001;V40:β=-0.41,95%CI为-0.60~-0.23,P<0.001)是辅助放疗LARC患者各个肠道受照剂量体积的独立影响因素,腹围(V10:β=-0.92,95%CI为-1.62~-0.22,P=0.010;V20:β=-0.84,95%CI为-1.11~-0.57,P<0.001;V30:β=-0.42,95%CI为-0.57~-0.28,P<0.001;V40:β=-0.30,95%CI为-0.41~-0.19,P<0.001)是新辅助放疗LARC患者各个肠道受照剂量体积的独立影响因素,腹围(OR=0.86,95%CI为0.78~0.95,P=0.002)是辅助放疗LARC患者急性肠道毒性的独立影响因素,腹围(OR=0.87,95%CI为0.79~0.96,P=0.004)是新辅助放疗LARC患者急性肠道毒性的独立影响因素。广义相加模型发现腹围与辅助放疗患者肠道受照剂量体积和急性肠道毒性存在非线性关系。进一步分段回归分析结果显示,腹围与肠道受照剂量体积(V10、V20、V30、V40)和急性肠道毒性间存在阈值效应,腹围与辅助放疗LARC患者肠道受照剂量体积V10、V20、V30、V40间的拐点值均为71.9 cm;腹围与新辅助放疗LARC患者肠道受照剂量体积V10、V20、V30、V40间的拐点值分别为69.0、69.0、69.0、68.6 cm;腹围与辅助放疗、新辅助放疗LARC患者急性肠道毒性的拐点值分别为71.9、69.0 cm。根据阈值95%CI上限将辅助和新辅助放疗患者的小腹围与中大腹围界值分别设定为76.1 cm和71.9 cm。在辅助放疗患者中,小腹围患者(n=22)不同水平肠道受照剂量体积V10[(7.65±2.29)cm3比(5.88±2.68)cm3,t=2.76,P=0.007]、V20[(4.28±1.27)cm3比(2.72±1.31)cm3,t=4.81,P<0.001]、V30[(2.42±1.07)cm3比(1.37±0.76)cm3,t=4.95,P<0.001]、V40[(1.69±0.74)cm3比(0.92±0.58)cm3,t=4.93,P<0.001]均显著高于中大腹围患者(n=60);在新辅助放疗患者中,小腹围患者(n=11)V20[(3.09±0.84)cm3比(2.28±1.17)cm3,t=2.17,P=0.033]、V30[1.44(1.22,1.53)cm3比0.91(0.56,1.22)cm3,Z=-3.04,P=0.002]、V40[0.93(0.84,1.09)cm3比0.44(0.30,0.81)cm3,Z=-3.19,P=0.001]均显著高于中大腹围患者(n=57)。在辅助放疗及新辅助放疗患者中,小腹围患者与中大腹围患者急性肠道毒性差异均有统计学意义(χ2 =10.46,P=0.001;χ2 =8.13,P=0.004)。结论 在标准模式下(俯卧位垫腹板并充盈膀胱),腹围是直肠癌放疗患者肠道受照剂量体积及急性放射性肠道毒性的独立影响因素。腹围与不同水平的肠道受照剂量体积和急性肠道毒性间存在明显的非线性阈值效应,在拐点值前后腹围对肠道受照剂量体积和毒性的影响存在显著差异。小腹围患者在现有标准放疗模式下不仅未获得预期获益,反而面临更高的肠道受照体积和毒性风险。