国际肿瘤学杂志 ›› 2026, Vol. 53 ›› Issue (3): 144-149.doi: 10.3760/cma.j.cn371439-20250415-00023
贺玉卿( ), 吴梓政, 齐铮琴
), 吴梓政, 齐铮琴
He Yuqing(), Wu Zizheng, Qi Zhengqin
摘要:
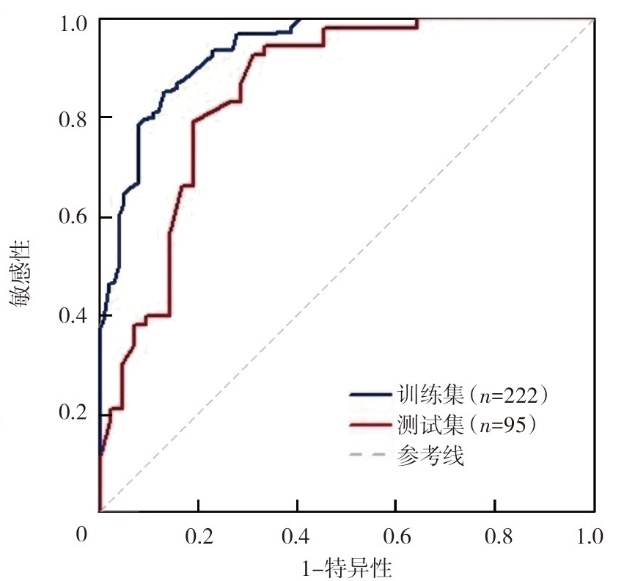
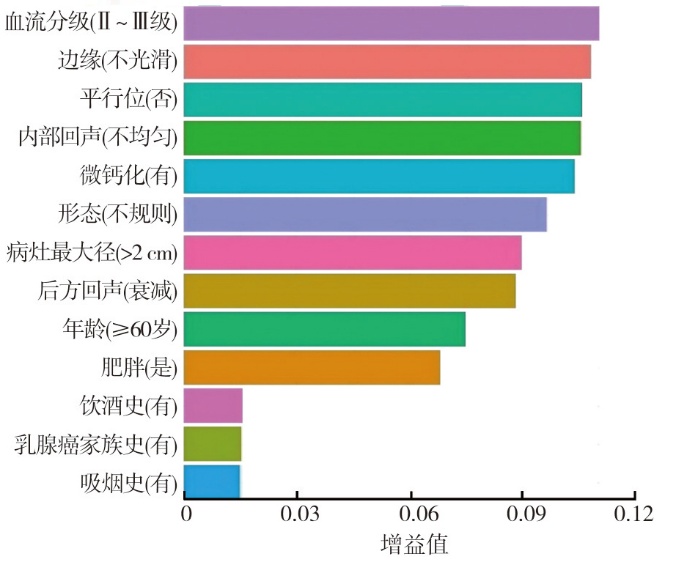
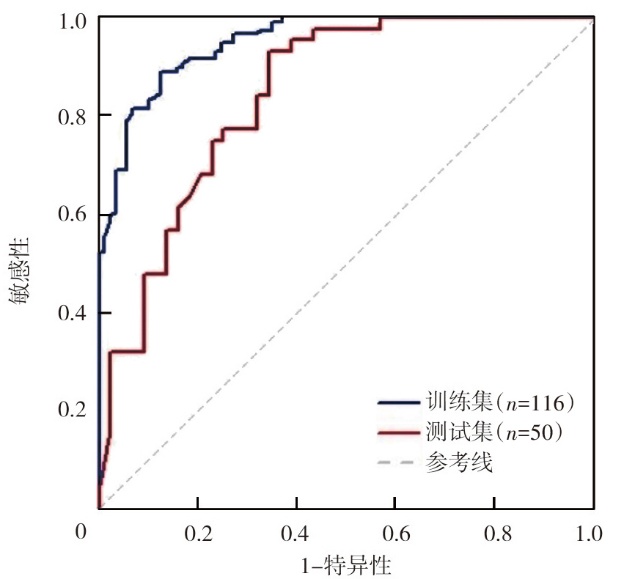
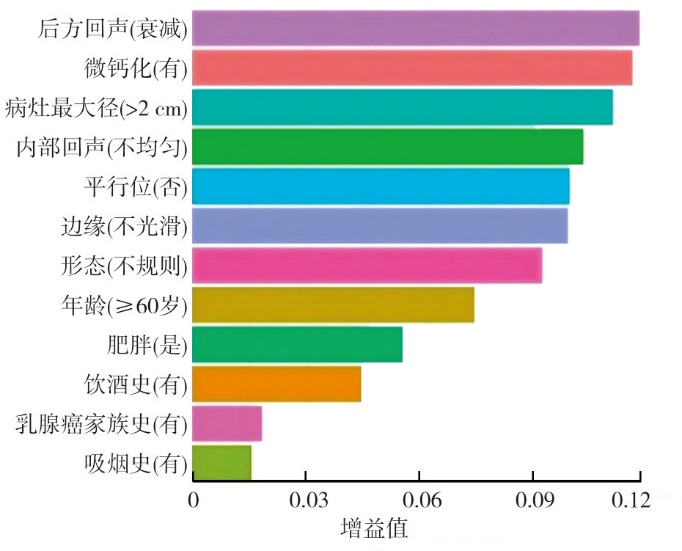
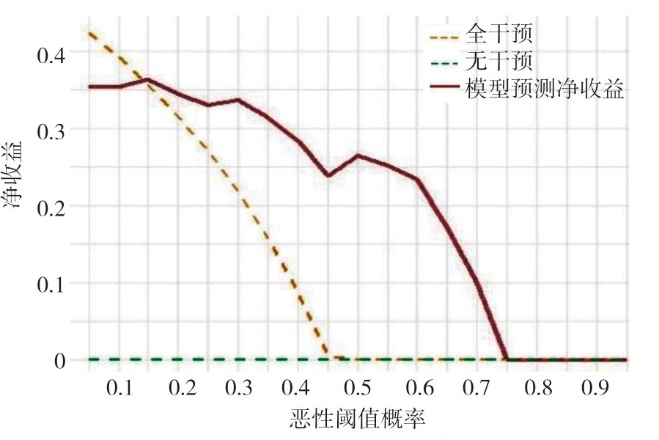
目的 基于临床和超声特征构建极端梯度提升(XGBoost)模型,评估模型预测低血流分级(Adler 0~Ⅰ级)乳腺影像报告与数据系统(BI-RADS)4类乳腺病变的恶性风险。方法 回顾性收集2023年6月至2024年12月于秦皇岛市第一医院诊断为BI-RADS 4类乳腺病变的317例女性患者的临床及超声资料(全样本),其中良性174例、恶性143例,采用7∶3随机分层抽样将患者分为训练集(n=222,良性122例、恶性100例)和测试集(n=95,良性52例、恶性43例);剔除高血流分级(Adler Ⅱ~Ⅲ级)患者后纳入低血流分级患者(低血流分级样本,n=166),同法按7∶3分为训练集(n=116,良性71例、恶性45例)和测试集(n=50,良性30例、恶性20例)。基于流行病学明确的乳腺癌风险因素(年龄、乳腺癌家族史、肥胖、饮酒史、吸烟史)及2013版ACR BI-RADS分类标准推荐的乳腺病变核心评估指标(血流分级、病灶最大径、微钙化、形态、边缘、内部回声、后方回声、平行位)构建预测BI-RADS 4类乳腺病变良、恶性的全样本XGBoost模型,剔除血流分级变量后余12项特征构建低血流分级XGBoost模型。采用受试者操作特征(ROC)曲线评估模型的预测效能,沙普利可加性解释(SHAP)分析明确模型特征贡献度,决策曲线分析(DCA)评估模型的准确性和实用性。结果 全样本中,良、恶性乳腺患者血流分级(χ²=4.99,P=0.026)、病灶最大径(χ²=4.47,P=0.034)、微钙化(χ²=7.10,P=0.009)、内部回声(χ²=4.24,P=0.041)、后方回声(χ²=22.32,P<0.001)分布差异均有统计学意义。ROC曲线分析显示,全样本训练集中XGBoost模型预测BI-RADS 4类乳腺病变良、恶性的曲线下面积(AUC)为0.936,95%CI为0.902~0.965,准确性为86.0%,敏感性为88.5%,特异性为83.2%;测试集AUC为0.852,95%CI为0.787~0.906,准确性为76.8%,敏感性为78.6%,特异性为75.0%。SHAP分析显示,血流分级(AdlerⅡ~Ⅲ级)对全样本XGBoost模型预测恶性风险的贡献最大,其次为边缘不光整、平行位否。低血流分级样本训练集中XGBoost模型预测BI-RADS 4类乳腺病变良、恶性的AUC为0.951,95%CI为0.917~0.975,准确性为86.5%,敏感性为87.9%,特异性为84.8%;测试集中AUC为0.843,95%CI为0.766~0.904,准确性为79.6%,敏感性为81.5%,特异性为77.8%。内部验证结果显示,XGBoost模型预测乳腺病变良、恶性的C-index为0.82。SHAP分析显示,后方回声衰减对低血流分级样本XGBoost模型预测恶性风险的正向贡献最大,其次为有微钙化、病灶最大径>2 cm、内部回声不均匀。DCA显示,该模型能提供较高的临床净获益,具有一定的临床实用性。结论 基于临床和超声特征的XGBoost模型可有效评估低血流分级BI-RADS 4类乳腺病变良、恶性,后方回声衰减、有微钙化、病灶最大径>2 cm、内部回声不均匀均为预测低血流分级BI-RADS 4类乳腺病变恶性风险的关键特征。