国际肿瘤学杂志 ›› 2021, Vol. 48 ›› Issue (1): 24-29.doi: 10.3760/cma.j.cn371439-20200728-00004
王浩澄, 董娅, 单东凤, 于壮( )
)
Wang Haocheng, Dong Ya, Shan Dongfeng, Yu Zhuang()
摘要:
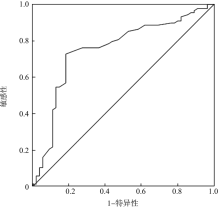
目的 探讨小细胞肺癌(SCLC)患者初治前血清胱抑素C与尿酸浓度对预后的影响。方法 选取2015年4月至2018年12月在青岛大学附属医院诊断为SCLC的患者196例,收集患者治疗前血清胱抑素C与尿酸等血液学指标。通过受试者工作特征(ROC)曲线确定胱抑素C与尿酸的最佳临界值。用Kaplan-Meier方法进行生存分析。采用Cox比例风险模型进行单因素、多因素分析。结果 患者治疗前血清胱抑素C与尿酸的最佳临界值分别为0.775 mg/L和296.45 μmol/L。生存分析显示,以最佳临界值为界,血清胱抑素C、尿酸浓度高的患者中位无进展生存时间(PFS)(5.49个月 vs. 8.57个月,χ2=35.943,P<0.001;6.67个月vs. 8.20个月,χ2=8.047,P=0.005)和总生存时间(OS)(13.37个月 vs. 23.95个月,χ2=21.355,P<0.001;14.13个月 vs. 20.97个月,χ2=11.333,P=0.001)均较浓度低的患者缩短。单因素分析显示,与PFS相关的因素有吸烟史(HR=0.707,95%CI为0.518~0.965,P=0.029)、分期(HR=1.776,95%CI为1.329~2.373,P<0.001)、一线化疗用药(HR=1.596,95%CI为1.072~2.376,P=0.021)、胸部放疗(HR=2.407,95%CI为1.803~3.214,P<0.001)、胱抑素C(HR=3.602,95%CI为1.716~7.561,P=0.001)、尿酸(HR=1.002,95%CI为1.000~1.003,P=0.036)及碱性磷酸酶(HR=1.010,95%CI为1.004~1.016,P=0.001);与OS相关的因素有吸烟史(HR=0.577,95%CI为0.382~0.870,P=0.009)、分期(HR=1.846,95%CI为1.295~2.630,P=0.001)、胸部放疗(HR=2.041,95%CI为1.426~2.921,P<0.001)、胱抑素C(HR=9.506,95%CI为3.278~27.564,P<0.001)及尿酸(HR=1.003,95%CI为1.001~1.005,P=0.006)。多因素分析显示,胸部放疗(HR=2.553,95%CI为1.774~3.672,P<0.001)、胱抑素C(HR=4.538,95%CI为1.875~10.982,P=0.001)及碱性磷酸酶(HR=1.011,95%CI为1.005~1.018,P=0.001)是PFS的独立预后因素;胱抑素C(HR=9.028,95%CI为2.680~30.413,P<0.001)是OS的独立预后因素。结论 SCLC患者治疗前血清胱抑素C与尿酸浓度均与患者预后有一定关系,浓度升高者PFS和OS缩短,预后差。治疗前血清胱抑素C浓度高可能提示患者病情进展快、生存时间较短,需注意疾病的进展与复发。