国际肿瘤学杂志 ›› 2020, Vol. 47 ›› Issue (4): 205-210.doi: 10.3760/cma.j.cn371439-20191210-00003
蒋婷婷, 徐晓婷, 秦颂兵, 马辰莺, 周菊英( )
)
Jiang Tingting, Xu Xiaoting, Qin Songbing, Ma Chenying, Zhou Juying()
摘要:
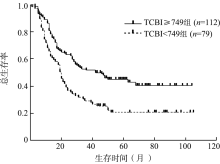
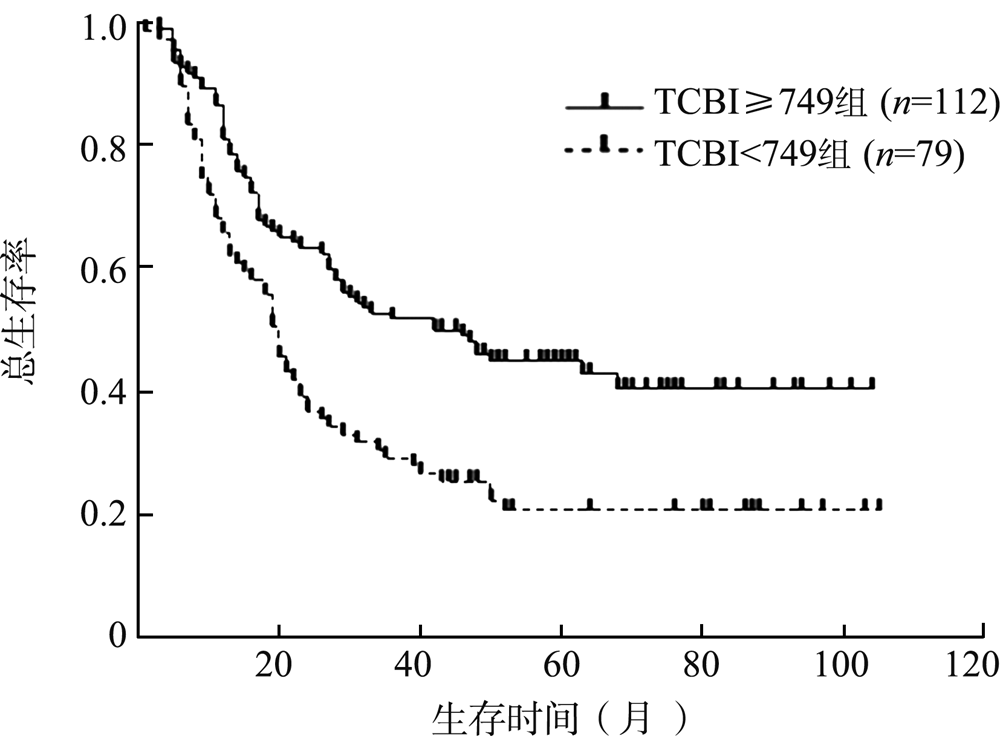
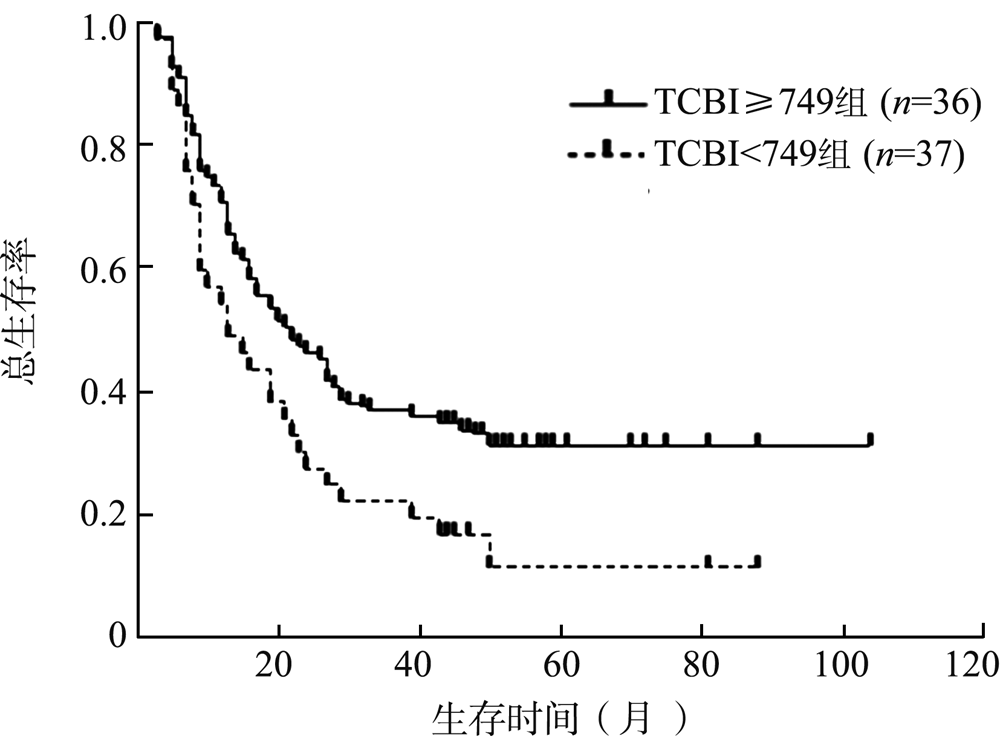
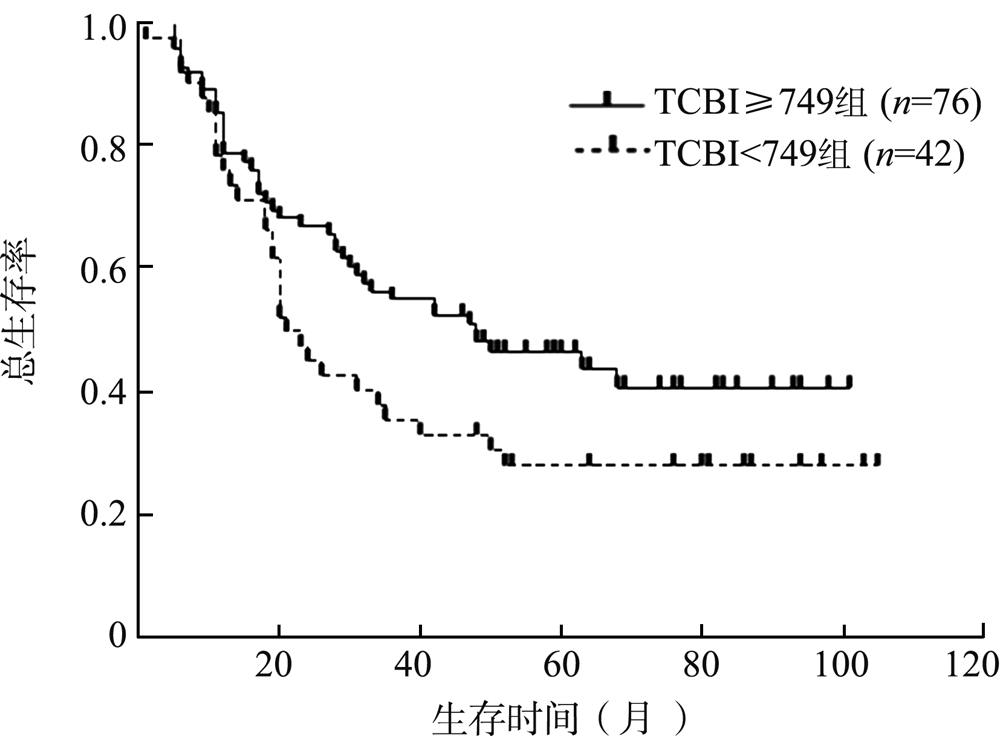
目的 探究TCBI对接受放疗的中老年胸段食管鳞状细胞癌(ESCC)患者的预后价值。方法 回顾性分析2010年1月至2015年12月于苏州大学附属第一医院肿瘤放疗科接受治疗的191例胸段ESCC患者的临床资料,根据入院时TCBI值[TCBI=血清甘油三酯(mg/dl)×总胆固醇(mg/dl)×体重(kg)/1 000]将患者分为TCBI低值组(n=79)和TCBI高值组(n=112)。分析TCBI与患者临床病理特征之间的关系。采用Kaplan-Meier法计算总生存期(OS),log-rank检验比较不同组别的生存差异,Cox比例风险模型分析影响中老年胸段ESCC患者放疗预后的因素,采用受试者工作特征(ROC)曲线验证TCBI在预后评估中的价值。结果 所有患者治疗前的TCBI为1 082±945。TCBI的临界值为749,<749为TCBI低值组;≥749为TCBI高值组。TCBI与患者的治疗方式(χ 2=4.235,P=0.040)和老年营养风险指数(GNRI,χ 2=8.795,P=0.003)相关。单因素分析结果提示,男性(HR=2.220,95%CI为1.223~4.030,P=0.009)、N1-3期(HR=1.453,95%CI为1.023~2.065,P=0.037)、GNRI<98(HR=1.949,95%CI为1.168~3.255,P=0.011)、TCBI<749(HR=1.846,95%CI为1.298~2.627,P=0.001)是影响中老年胸段ESCC患者OS的危险因素,术后辅助放疗(HR=0.641,95%CI为0.449~0.915,P=0.014)是其保护因素。多因素分析结果提示,男性(HR=2.147,95%CI为1.173~3.929,P=0.013)、TCBI<749(HR=1.664,95%CI为1.166~2.376,P=0.005)是影响中老年胸段ESCC患者OS的独立危险因素,术后辅助放疗(HR=0.630,95%CI为0.439~0.903,P=0.012)是其独立保护因素。ROC曲线计算得到曲线下面积为0.619,敏感性为0.742,特异性为0.496(P=0.007),肯定了TCBI在预后评估中的作用。生存分析结果显示,TCBI高值组患者中位OS为42个月,1年和3年生存率分别为86.6%、52.7%,明显好于TCBI低值组(中位OS为20个月,1年生存率68.4%,3年生存率29.1%;χ 2=12.286,P<0.001)。亚组分析结果显示,接受根治性放疗的患者中,TCBI低值的患者(n=37)3年生存率低于TCBI高值的患者(n=36)(21.6% vs. 44.4%,χ 2=8.505,P=0.004)。结论 治疗前TCBI是中老年胸段ESCC患者放疗后OS的预测指标,TCBI越低,患者生存预后越差。