国际肿瘤学杂志 ›› 2020, Vol. 47 ›› Issue (5): 278-283.doi: 10.3760/cma.j.cn371439-20190930-00018
郭信伟1, 冀胜军2, 姬磊3, 张晗4, 周绍兵1( ), 刘阳晨1
), 刘阳晨1
Guo Xinwei1, Ji Shengjun2, Ji Lei3, Zhang Han4, Zhou Shaobing1(), Liu Yangchen1
摘要:
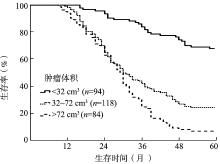
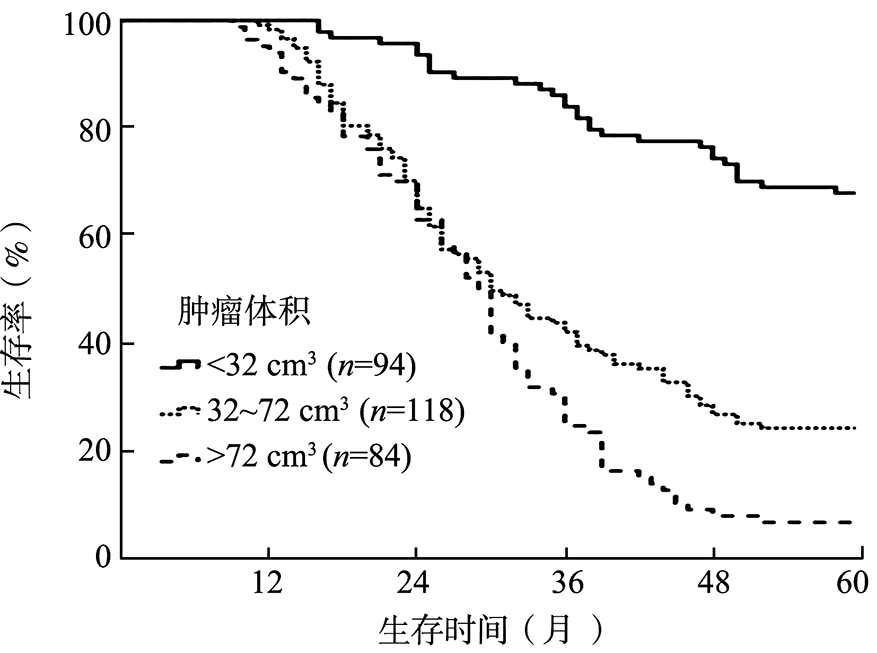
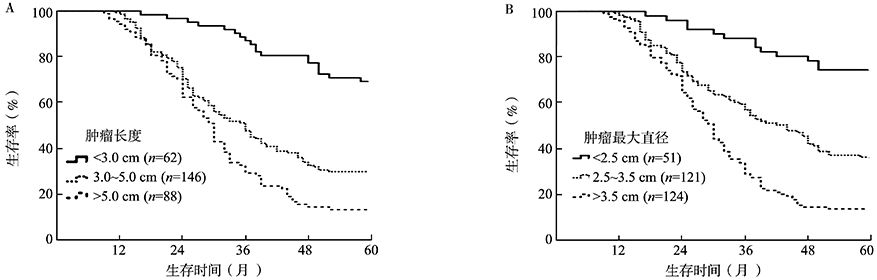
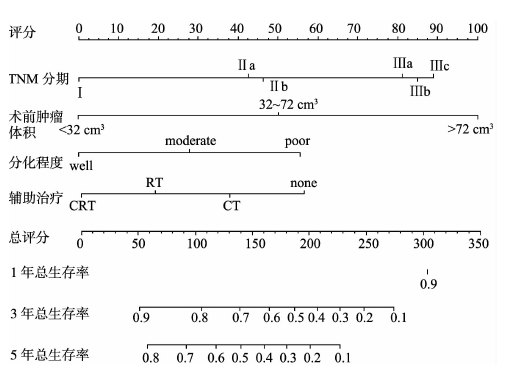
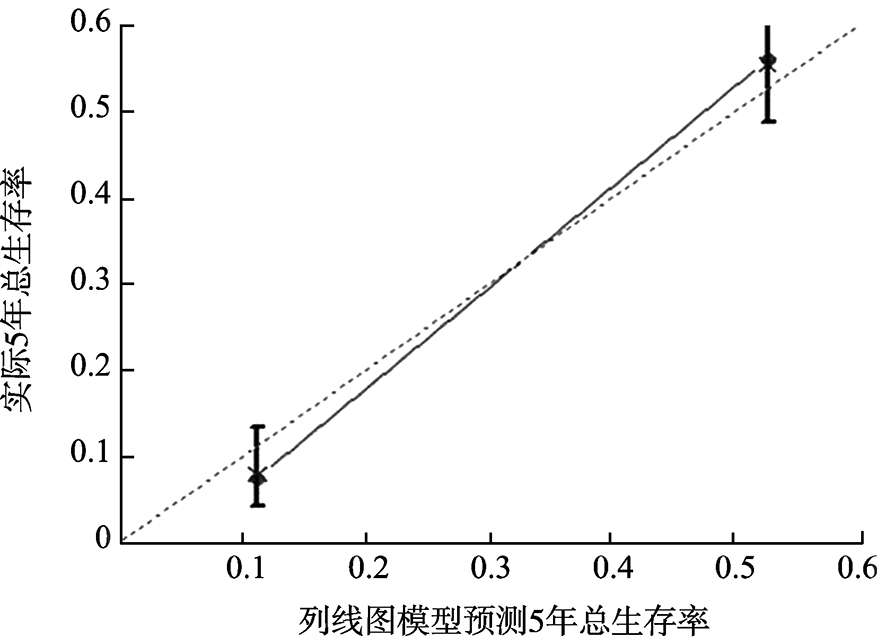
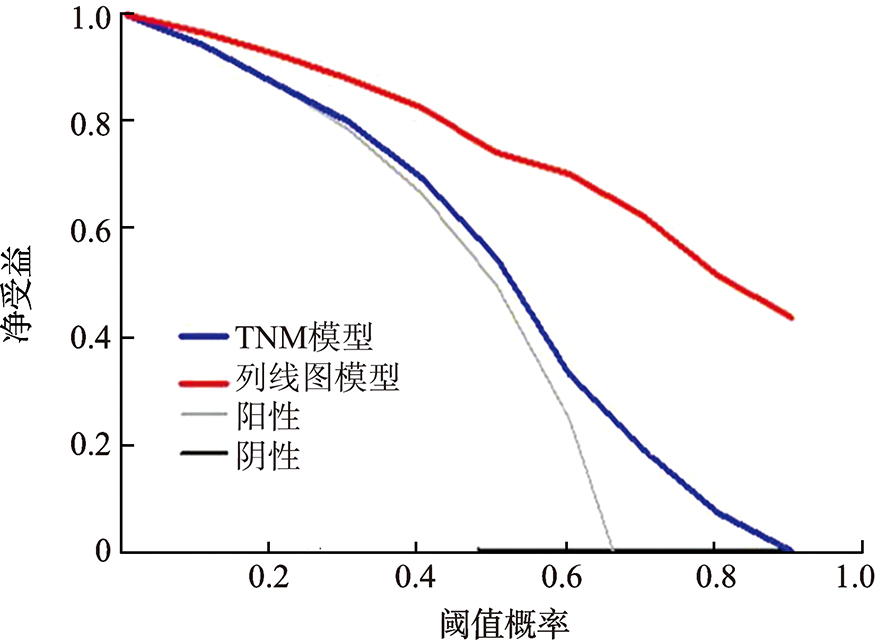
目的 探索除TNM分期外的临床病理因素,包括术前肿瘤体积、长度及最大直径对胸段食管鳞状细胞癌预后的影响,并以列线图(nomogram)的方式评价有统计学意义的临床病理变量预测总生存率的情况。方法 回顾性分析2011—2014年在扬州大学附属泰兴人民医院胸外科接受食管癌根治术的296例患者,根据术前肿瘤体积、长度及最大直径的最佳临界值进行分组,采用Kaplan-Meier法计算生存率并行log-rank检验,应用Cox模型单因素及多因素分析临床变量与生存预后的关系,最终纳入有统计学意义的临床病理参数建立列线图模型,并通过校准曲线图、一致性指数(C-index)和决策曲线图进一步验证该模型的预测价值。结果 经X-tile分析确定术前肿瘤体积的最佳临界值为32 cm 3和72 cm 3,肿瘤体积<32 cm 3(n=94)、32~72 cm 3(n=118)和>72 cm 3(n=84)的3组患者1、3、5年生存率分别为100%、84.0%、68.1%,98.3%、42.4%、24.6%和94.1%、25.0%、7.1%(χ 2=86.639,P<0.001);肿瘤长度的最佳临界值为3.0 cm和5.0 cm,肿瘤长度<3.0 cm(n=62)、3.0~5.0 cm(n=146)和>5.0 cm(n=88)的3组患者1、3、5年生存率分别为99.5%、87.1%、69.4%,98.6%、47.9%、30.1%和94.3%、29.6%、13.6%(χ 2=53.607,P<0.001);肿瘤最大直径的最佳临界值为2.5 cm和3.5 cm,肿瘤最大直径<2.5 cm(n=51)、2.5~3.5 cm(n=121)和>3.5 cm(n=124)的3组患者1、3、5年生存率分别为99.5%、84.3%、74.5%,98.3%、57.0%、36.4%和96.0%、29.0%、13.7%(χ 2=62.109,P<0.001)。单因素分析结果显示,肿瘤位置、分化程度、T分期、N分期、TNM分期、辅助治疗、术前肿瘤体积、长度及最大直径均与胸段食管鳞状细胞癌患者的总生存期(OS)密切相关(均P<0.05)。Cox多因素分析结果显示,分化程度(HR=0.514,95%CI为0.366~0.723,P=0.019)、TNM分期(HR=1.757,95%CI为1.267~2.612,P=0.015)、辅助治疗(HR=0.669,95%CI为0.503~0.889,P=0.006)和术前肿瘤体积(将<32 cm 3设为哑变量,32~72 cm 3:HR=3.689,95%CI为2.415~5.637,P<0.001;>72 cm 3:HR=5.720,95%CI为3.606~9.075,P<0.001)是影响OS的独立危险因素。根据多变量分析有统计学意义的临床病理参数而构建的列线图模型预测胸段食管鳞状细胞癌术后OS的C-index为0.722(95%CI为0.687~0.757),明显高于第7版AJCC TNM分期的C-index(0.633,95%CI为0.595~0.671)。另外,校准曲线图表明列线图模型预测5年OS率和实际观察值之间存在高度一致性,决策曲线分析也表明,列线图模型预测胸段食管鳞状细胞癌术后的生存预后比TNM分期模型具有更高的临床应用潜能。结论 纳入术前肿瘤体积的列线图在预测胸段食管鳞状细胞癌患者生存预后方面具有重要价值。