国际肿瘤学杂志 ›› 2020, Vol. 47 ›› Issue (11): 675-681.doi: 10.3760/cma.j.cn371439-20191224-00099
宋明泽1, 程一鸣1, 李刚2, 王振明2, 李世荣2( )
)
Song Mingze1, Cheng Yiming1, Li Gang2, Wang Zhenming2, Li Shirong2()
摘要:
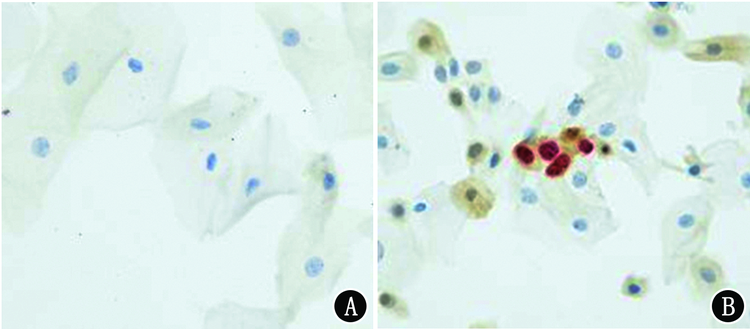
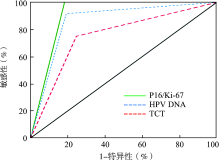
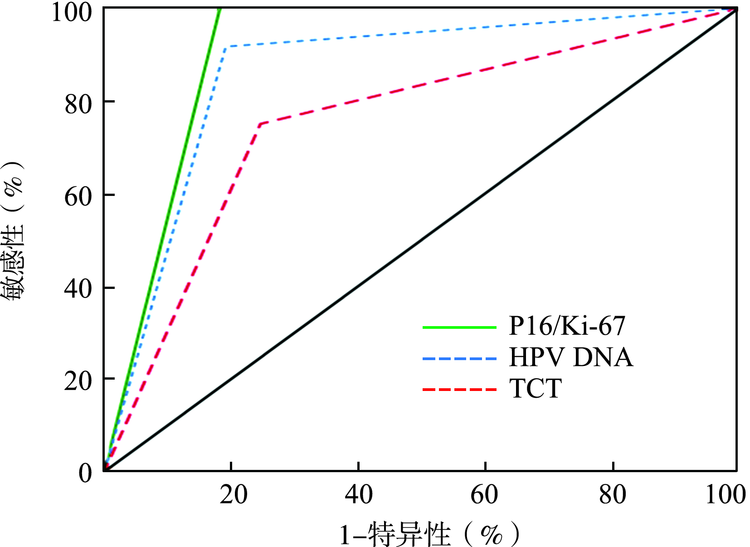
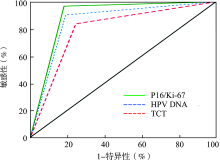
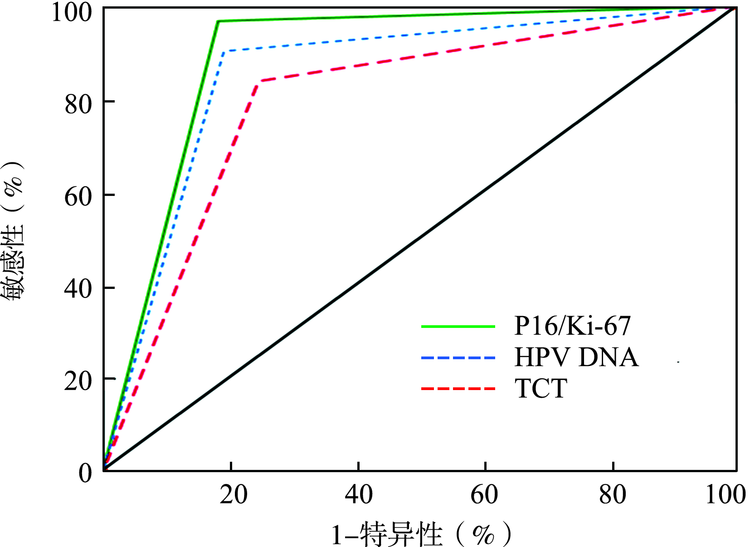
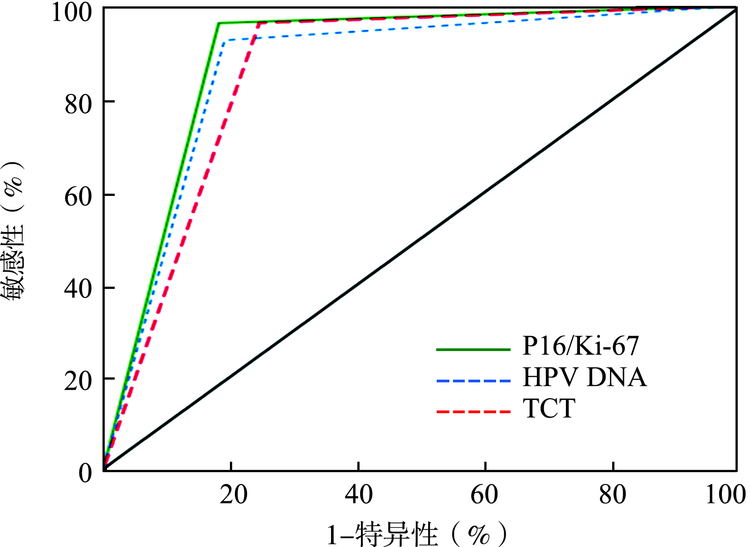
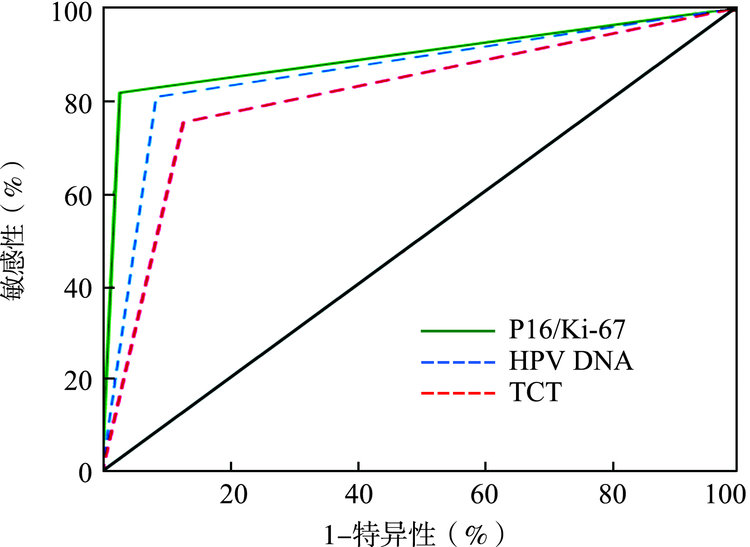
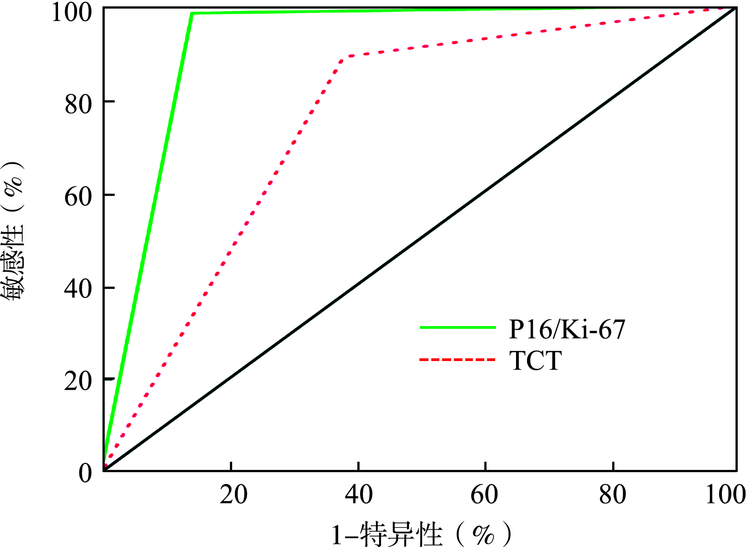
目的 探讨P16/Ki-67双染检测技术在宫颈癌及癌前病变筛查中的价值和临床意义。方法 选取2018年9月至2019年5月山东省潍坊市人民医院妇科收治的110例宫颈上皮内瘤变(CIN)2级以下的患者、31例CIN2级患者、27例CIN3级患者和12例宫颈癌患者,分别评估人乳头瘤病毒(HPV)DNA、液基细胞学技术(TCT)和P16/Ki-67双染检测作为宫颈癌及癌前病变初筛方法的敏感性、特异性、阳性预测值和阴性预测值,并探讨P16/Ki-67双染检测技术用作高危型HPV阳性患者分流的可行性。结果 HPV DNA、TCT和P16/Ki-67双染检测诊断<CIN2级的敏感性分别为80.91%、75.45%、81.82%,特异性分别为91.43%、87.14%、97.14%,阳性预测值分别为93.68%、90.22%、97.83%,阴性预测值分别为75.29%、69.32%、77.27%,差异均具有统计学意义(χ2=1.593,P=0.042;χ2=4.736,P=0.034;χ2=4.667,P=0.037;χ2=1.564,P=0.048),P16/Ki-67双染检测的特异性高于HPV DNA及TCT,敏感性及阳性预测值均高于TCT(均P<0.012 5)。3种方法诊断CIN2级的敏感性分别为90.32%、83.87%、96.77%,差异具有统计学意义(χ2=2.952,P=0.029);特异性分别为80.91%、75.45%、81.82%,差异无统计学意义(χ2=2.505,P=0.066);阳性预测值分别为57.10%、49.10%、60.00%,差异无统计学意义(χ2=1.939,P=0.079);阴性预测值分别为96.70%、94.30%、98.90%,差异具有统计学意义(χ2=3.175,P=0.013);P16/Ki-67双染检测的敏感性、阴性预测值均高于TCT(均P<0.012 5)。3种方法诊断CIN3级的敏感性分别为92.59%、96.30%、96.30%,差异无统计学意义(χ2=0.497,P=0.780);特异性分别为80.91%、75.45%、81.82%,差异具有统计学意义(χ2=4.677,P=0.036);阳性预测值分别为54.30%、49.10%、56.50%,差异具有统计学意义(χ2=1.760,P=0.045);阴性预测值分别为97.80%、98.80%、98.90%,差异无统计学意义(χ2=0.441,P=0.802);P16/Ki-67双染检测的特异性、阳性预测值均高于TCT(均P<0.012 5)。3种方法诊断宫颈癌的敏感性分别为91.67%、75.00%、100.00%,差异具有统计学意义(χ2=3.293,P=0.034);特异性分别为80.91%、75.45%、81.82%,阳性预测值分别为34.40%、25.00%、37.50%,阴性预测值分别为98.90%、96.50%、100.00%,差异均无统计学意义(χ2=2.736,P=0.255;χ2=1.834,P=0.400;χ2=3.075,P=0.081);P16/Ki-67双染检测的敏感性高于TCT(P<0.012 5)。针对高危型HPV阳性患者的分流,P16/Ki-67双染检测及TCT诊断的敏感性分别为98.44%、89.06%,特异性分别为85.71%、61.90%,阴性预测值分别为94.70%、65.00%,差异均具有统计学意义(χ2=4.800,P=0.028;χ2=3.079,P=0.039;χ2=5.284,P=0.022);阳性预测值分别为95.50%、87.70%,差异无统计学意义(χ2=2.565,P=0.109)。结论 细胞学P16/Ki-67双染检测诊断<CIN2级的特异性高于HPV DNA及TCT,敏感性及阳性预测值高于TCT;诊断CIN2级的敏感性、阴性预测值均高于TCT;诊断CIN3级的特异性、阳性预测值均高于TCT;诊断宫颈癌的敏感性高于TCT。在对高危型HPV阳性患者的分流当中,P16/Ki-67双染检测提供了一种更加灵敏和准确的分流路径。