Journal of International Oncology ›› 2026, Vol. 53 ›› Issue (7): 412-419.doi: 10.3760/cma.j.cn371439-20251019-00067
• Original Article • Previous Articles Next Articles
Predictive value of XGBoost model for pathological complete response after neoadjuvant chemotherapy in breast cancer patients
Liu Yonghong, Zhang Bo, Xue Lingbo, Hu Pengfei, Zhang Zhenyu, Li Jie( )
)
Department of Thyroid and Breast Surgery ,Cangzhou Central Hospital of Hebei Province Cangzhou 061000, China
-
Received:2025-10-19Online:2026-07-08Published:2026-06-25 -
Contact:Li Jie E-mail:lj13513279709@hotmail.com -
Supported by:Scientific and Technological Project of Cangzhou of China(222106087)
Cite this article
Liu Yonghong, Zhang Bo, Xue Lingbo, Hu Pengfei, Zhang Zhenyu, Li Jie. Predictive value of XGBoost model for pathological complete response after neoadjuvant chemotherapy in breast cancer patients[J]. Journal of International Oncology, 2026, 53(7): 412-419.
share this article
"
| 临床资料 | 内部数据集 | 外部验证集 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非pCR(n=142) | pCR(n=30) | χ2值 | P值 | 非pCR(n=34) | pCR(n=7) | χ2值 | P值 | ||||||||||
| 年龄(岁) | |||||||||||||||||
| <55 | 91(64.08) | 17(56.67) | 0.58 | 0.445 | 21(61.76) | 5(71.43) | <0.01 | 0.958 | |||||||||
| ≥55 | 51(35.92) | 13(43.33) | 13(38.24) | 2(28.57) | |||||||||||||
| 月经状态 | |||||||||||||||||
| 绝经前 | 67(47.18) | 16(53.33) | 0.38 | 0.540 | 23(67.65) | 6(85.71) | 0.25 | 0.617 | |||||||||
| 绝经后 | 75(52.82) | 14(46.67) | 11(32.35) | 1(14.29) | |||||||||||||
| 肿瘤长径(cm) | |||||||||||||||||
| <5 | 58(40.85) | 19(63.33) | 5.07 | 0.024 | 18(52.94) | 5(71.43) | 0.23 | 0.632 | |||||||||
| ≥5 | 84(59.15) | 11(36.67) | 16(47.06) | 2(28.57) | |||||||||||||
| 腋窝淋巴结状态 | |||||||||||||||||
| 阴性 | 77(54.23) | 26(86.67) | 10.85 | <0.001 | 17(50.00) | 7(100) | 4.10 | 0.043 | |||||||||
| 阳性 | 65(45.77) | 4(13.33) | 17(50.00) | 0(0) | |||||||||||||
| ER | |||||||||||||||||
| 阴性 | 57(40.14) | 16(53.33) | 1.77 | 0.184 | 16(47.06) | 4(57.14) | 0.01 | 0.943 | |||||||||
| 阳性 | 85(59.86) | 14(46.67) | 18(52.94) | 3(42.86) | |||||||||||||
| PR | |||||||||||||||||
| 阴性 | 61(42.96) | 17(56.67) | 1.88 | 0.171 | 16(47.06) | 4(57.14) | 0.01 | 0.943 | |||||||||
| 阳性 | 81(57.04) | 13(43.33) | 18(52.94) | 3(42.86) | |||||||||||||
| HER2 | |||||||||||||||||
| 阴性 | 76(53.52) | 22(73.33) | 3.97 | 0.046 | 20(58.82) | 2(28.57) | 1.09 | 0.296 | |||||||||
| 阳性 | 66(46.48) | 8(26.67) | 14(41.18) | 5(71.43) | |||||||||||||
| Ki-67表达 | |||||||||||||||||
| ≤20% | 50(35.21) | 4(13.33) | 5.50 | 0.019 | 13(38.24) | 0(0) | 2.35 | 0.125 | |||||||||
| >20% | 92(64.79) | 26(86.67) | 21(61.76) | 7(100) | |||||||||||||
| 组织学分级 | |||||||||||||||||
| 1~2级 | 94(66.20) | 24(80.00) | 2.19 | 0.139 | 18(52.94) | 6(85.71) | 1.40 | 0.237 | |||||||||
| 3级 | 48(33.80) | 6(20.00) | 16(47.06) | 1(14.29) | |||||||||||||
| 新辅助化疗方案 | |||||||||||||||||
| 蒽环类 | 9(6.34) | 3(10.00) | 1(2.94) | 0(0) | |||||||||||||
| 紫杉醇类 | 13(9.15) | 7(23.33) | 0.047 | 3(8.82) | 2(28.57) | 0.361 | |||||||||||
| 蒽环类+紫杉醇类 | 120(84.51) | 20(66.67) | 30(88.24) | 5(71.43) | |||||||||||||
| 靶向治疗 | |||||||||||||||||
| 是 | 9(6.34) | 6(20.00) | 4.22 | 0.040 | 2(5.88) | 1(14.29) | 0.439 | ||||||||||
| 否 | 133(93.66) | 24(80.00) | 32(94.12) | 6(85.71) | |||||||||||||
"
| 因素 | OR值 | 95%CI | P值 |
|---|---|---|---|
| 年龄(≥55岁/<55岁) | 1.27 | 0.51~3.18 | 0.613 |
| 月经状态(绝经后/绝经前) | 1.09 | 0.44~2.71 | 0.851 |
| 肿瘤长径(≥5 cm/<5 cm) | 2.84 | 1.10~7.32 | 0.031 |
| 腋窝淋巴结状态(阳性/阴性) | 4.80 | 1.34~17.21 | 0.016 |
| ER(阳性/阴性) | 1.38 | 0.55~3.48 | 0.489 |
| PR(阳性/阴性) | 1.45 | 0.58~3.61 | 0.428 |
| HER2(阳性/阴性) | 0.49 | 0.19~1.31 | 0.156 |
| Ki-67表达(≤20%/>20%) | 4.04 | 1.12~14.55 | 0.032 |
| 组织学分级(3级/1~2级) | 1.12 | 0.99~1.26 | 0.063 |
| 新辅助化疗方案(蒽环类+ 紫杉醇类/紫杉醇类或蒽环类) | 1.06 | 1.00~1.12 | 0.072 |
| 靶向治疗(是/否) | 0.15 | 0.04~0.56 | 0.004 |
"
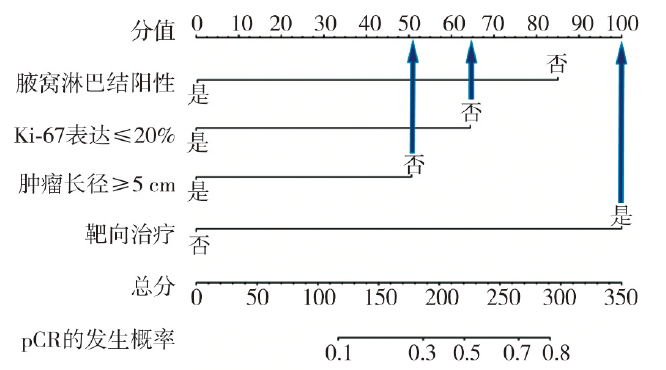
| 因素 | OR值 | 95%CI | P值 |
|---|---|---|---|
| 肿瘤长径(≥5 cm/<5 cm) | 3.32 | 1.12~9.91 | 0.031 |
| 腋窝淋巴结状态(阳性/阴性) | 7.86 | 1.83~33.63 | 0.005 |
| Ki-67表达(≤20%/>20%) | 4.84 | 1.16~20.25 | 0.031 |
| 靶向治疗(是/否) | 0.11 | 0.02~0.60 | 0.011 |
"
"
"

"
"
"
"
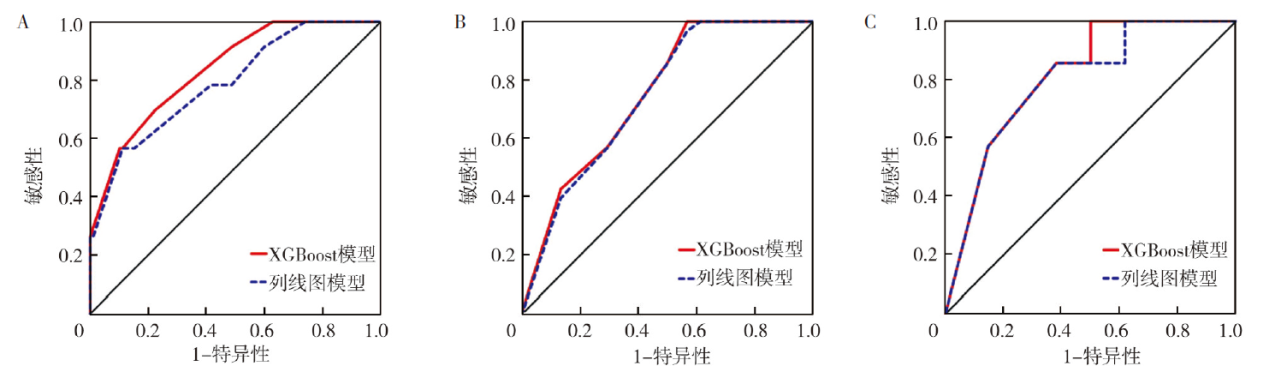
| 模型 | AUC | 95%CI | 敏感性(%) | 特异性(%) |
|---|---|---|---|---|
| 内部训练集(n=121) | ||||
| XGBoost模型 | 0.84 | 0.75~0.92 | 69.6 | 77.6 |
| 列线图模型 | 0.79 | 0.69~0.89 | 56.5 | 88.8 |
| 内部验证集(n=51) | ||||
| XGBoost模型 | 0.75 | 0.58~0.91 | 100 | 43.1 |
| 列线图模型 | 0.70 | 0.50~0.90 | 100 | 29.5 |
| 外部验证集(n=41) | ||||
| XGBoost模型 | 0.81 | 0.66~0.96 | 100 | 50.0 |
| 列线图模型 | 0.79 | 0.62~0.97 | 85.7 | 61.8 |
| [1] | Lan T, Lu YY, He JW, et al. Global, reginal, national burden and risk factors in female breast cancer from 1990 to 2021[J]. iScience, 2024, 27(10): 111045. DOI: 10.1016/j.isci.2024.111045. |
| [2] | Grindrod N, Cecchini M, Brackstone M. Concurrent neoadjuvant chemotherapy and radiation in locally advanced breast cancer: impact on locoregional recurrence rates[J]. Curr Oncol, 2025, 32(2): 85. DOI: 10.3390/curroncol32020085. |
| [3] | Bozer A, Yilmaz C, Çetin Tunçez H, et al. Correlation of histopathological and radiological response patterns and their prognostic implications in breast cancer after neoadjuvant chemotherapy[J]. Breast Cancer (Dove Med Press), 2024, 16: 1005-1017. DOI: 10.2147/bctt.S495553. |
| [4] | Deleon A, Murala A, Decker I, et al. Machine learning-based prediction of mortality in pediatric trauma patients[J]. Front Pediatr, 2025, 13: 1522845. DOI: 10.3389/fped.2025.1522845. |
| [5] | Li XY, Zhou ZY, Zhang XY, et al. Predicting 3-year all-cause mortality in rectal cancer patients based on body composition and machine learning[J]. Front Nutr, 2025, 12: 1473952. DOI: 10.3389/fnut.2025.1473952. |
| [6] | AJCC. AJCC cancer staging manual[M]. 6th ed. New York: Springer, 2002. |
| [7] | 中国抗癌协会乳腺癌专业委员会, 中华医学会肿瘤学分会乳腺肿瘤学组. 中国抗癌协会乳腺癌诊治指南与规范(2026年版)[J]. 中国癌症杂志, 2025, 35(12): 1157-1255. DOI: 10.19401/j.cnki.1007-3639.2025.12.009. |
| [8] | Chen XW, Ye HM, Xu DM, et al. Pathological complete response and prognostic predictive factors of neoadjuvant chemoimmunotherapy in early stage triple-negative breast cancer[J]. Front Immunol, 2025, 16: 1570394. DOI: 10.3389/fimmu.2025.1570394. |
| [9] | Yuan SF, Zhu LJ, Chen XQ, et al. Huanglian Jiedu Tang regulates the inflammatory microenvironment to alleviate the progression of breast cancer by inhibiting the RhoA/ROCK pathway[J]. Tissue Cell, 2025, 95: 102850. DOI: 10.1016/j.tice.2025.102850. |
| [10] |
Häberle L, Erber R, Gass P, et al. Prediction of pathological complete response after neoadjuvant chemotherapy for HER2-negative breast cancer patients with routine immunohistochemical markers[J]. Breast Cancer Res, 2025, 27(1): 13. DOI: 10.1186/s13058-025-01960-8.
pmid: 39856787 |
| [11] | Ebaid NF, Abdelkawy KS, Said ASA, et al. Is the neutrophil-to-lymphocyte ratio a predictive factor of pathological complete response in egyptian breast cancer patients treated with neoadjuvant chemotherapy?[J]. Medicina (Kaunas), 2025, 61(2): 327. DOI: 10.3390/medicina61020327. |
| [12] | Pan FQ, Wang YL, Zhang BQ, et al. Early peritumoral edema change improve prediction of pathological complete response in breast cancer: a multiparametric magnetic resonance imaging-based model[J]. Front Oncol, 2026, 16: 1671985. DOI: 10.3389/fonc.2026.1671985. |
| [13] |
Yan D, Xie JW, Cheng WL, et al. Ultrasound-based radiomic nomogram for predicting the invasive status of breast cancer: a multicenter study[J]. Eur J Med Res, 2025, 30(1): 526. DOI: 10.1186/s40001-025-02828-5.
pmid: 40598678 |
| [14] |
Duan S, Aisimutula D, Wang YY, et al. Factors influencing the efficacy of neoadjuvant chemotherapy for HER-2-low early-stage breast cancer and a predictive model for pathological complete response[J]. Gland Surg, 2025, 14(8): 1418-1432. DOI: 10.21037/gs-2025-7.
pmid: 40948929 |
| [15] |
Lv YL, Mu WM, Yang QZ, et al. Nomogram for predicting pathological complete response after neoadjuvant chemotherapy in operable primary breast cancer[J]. J Coll Physicians Surg Pak, 2025, 35(3): 324-330. DOI: 10.29271/jcpsp.2025.03.324.
pmid: 40055167 |
| [16] | Akdag G, Yildirim S, Dogan A, et al. Neoadjuvant chemotherapy and pathologic complete response in HR+/HER2- breast cancer: impact of tumor Ki67 and ER status[J]. Chemotherapy, 2024, 69(3): 141-149. DOI: 10.1159/000537874. |
| [17] | Toli MA, Liu XR, Massa D, et al. Prognostic significance of tumour Ki-67 dynamics during neoadjuvant treatment in patients with breast cancer: a population-based cohort study[J]. Lancet Reg Health Eur, 2025, 58: 101432. DOI: 10.1016/j.lanepe.2025.101432. |
| [18] | Fang S, Xia WJ, Zhang HB, et al. A real-world clinicopathological model for predicting pathological complete response to neoadjuvant chemotherapy in breast cancer[J]. Front Oncol, 2024, 14: 1323226. DOI: 10.3389/fonc.2024.1323226. |
| [19] | 杨静, 余瑶. dNLR、MRR对乳腺癌患者新辅助化疗疗效的评估价值[J]. 检验医学与临床, 2023, 20(19): 2863-2867. DOI: 10.3969/j.issn.1672-9455.2023.19.020. |
| [20] | 王智宝, 李广现, 张昕昕, 等. MRI联合血清lncRNA KCNQ1OT1、miR-204-5p对乳腺癌腋窝淋巴结转移的预测价值[J]. 国际肿瘤学杂志, 2025, 52(2): 89-93. DOI: 10.3760/cma.j.cn371439-20240727-00013. |
| [21] |
Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort[J]. Lancet, 2010, 375(9712): 377-384. DOI: 10.1016/s0140-6736(09)61964-4.
pmid: 20113825 |
| [22] |
Gianni L, Pienkowski T, Im YH, et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (Neo Sphere): a multicentre, open-label, phase 2 randomised trial[J]. Lancet Oncol, 2016, 17(6): 791-800. DOI: 10.1016/s1470-2045(16)00163-7.
pmid: 27179402 |
| [23] | Fang YT, Zhang QC, Wu Y, et al. HER2-positive is an independent indicator for predicting pathological complete response to neoadjuvant therapy and Ki67-changed after neoadjuvant chemotherapy predicts favorable prognosis in Chinese women with locally advanced breast cancer[J]. Medicine (Baltimore), 2024, 103(6): e37170. DOI: 10.1097/md.0000000000037170. |
| [24] | D'Anna A, Aranzulla C, Carnaghi C, et al. Comparative analysis of machine learning models for predicting pathological complete response to neoadjuvant chemotherapy in breast cancer: an MRI radiomics approach[J]. Phys Med, 2025, 131: 104931. DOI: 10.1016/j.ejmp.2025.104931. |
| [25] |
Zheng GY, Peng JX, Shu ZY, et al. Predicting pathological complete response to neoadjuvant chemotherapy in breast cancer patients: use of MRI radiomics data from three regions with multiple machine learning algorithms[J]. J Cancer Res Clin Oncol, 2024, 150(3): 147. DOI: 10.1007/s00432-024-05680-y.
pmid: 38512406 |
| [1] | Su Jialin, Zheng Jin, Zhao Canjun, Han Lijun, Zhang Jie, Wang Liping. Factors influencing the occurrence of high-grade acute radiodermatitis in patients undergoing image guided radiation therapy after breast cancer surgery and the construction of a prediction model [J]. Journal of International Oncology, 2026, 53(6): 339-345. |
| [2] | Gu Lei, Han Jihua, Tian Wenze, Zhou Wubi, Xin Yong. Correlation between the changes in sPD-1 after neoadjuvant therapy in patients with esophageal squamous cell carcinoma and pathological response [J]. Journal of International Oncology, 2026, 53(5): 276-282. |
| [3] | Li Lina, Liu Shuai, Zhang Nan. Research progress on preoperative radiotherapy for breast cancer [J]. Journal of International Oncology, 2026, 53(5): 301-305. |
| [4] | Li Yao, Tian Lin, Liu Haolin, Xiao Jing. Effects of lncRNA CASC19 on proliferation,migration and invasion of breast cancer cells by regulating miR-410-3p/LAMC1 signaling pathway [J]. Journal of International Oncology, 2026, 53(3): 129-136. |
| [5] | Liu Xinlei, Li Yaru, Chen Shuning, Tang Shenghao, Qin Yan, Liu Yankui, Qi Xiaowei. Research progress of HER2 ultra-low expression breast cancer [J]. Journal of International Oncology, 2026, 53(1): 53-56. |
| [6] | Chen Qiaoliang, Qin Xinyan, Lai Ruihe, Tan Shuangxiu. Diagnostic value of multimodal Nomogram model combining 18F-FDG PET/CT and ultrasound for triple negative breast cancer [J]. Journal of International Oncology, 2025, 52(9): 560-565. |
| [7] | Guo Junlong, Zou Ruiqi, Chen Shaoqiang, Liang Yuxin, Li Jing, Yong Sunan, He Yuting, Xie Xiaobing, Li Ping. Research progress of RNA m6A modification in breast cancer [J]. Journal of International Oncology, 2025, 52(8): 532-537. |
| [8] | Li Chengqiang, Wang Yungang, Yu Yishan, Wu Shizhang, Tao Cheng, Ma Xingmin, Dai Tianyuan, Duan Jinghao, Chen Jinhu, Bai Tong, Zhu Jian. Analysis of dosimetric characteristics of proton radiotherapy in 4 cases of breast cancer [J]. Journal of International Oncology, 2025, 52(7): 448-454. |
| [9] | Li Lixi, Duan Boshi, Qian Haili, Ma Fei. Advances in the clinical and translational applications of breast cancer organoids [J]. Journal of International Oncology, 2025, 52(6): 379-381. |
| [10] | Zhou Wenkao, Huang Hesen, Pan Yimei, Huang Lingyan, Wang Mingshan, Zhao Fangli, Wang Ya, Tang Huimin. Comparison of the efficacy and construction of prediction model for relapse free survival in breast cancer based on diabetes mellitus type 2 [J]. Journal of International Oncology, 2025, 52(5): 295-303. |
| [11] | Wang Zhibao, Li Guangxian, Zhang Xinxin, Cui Wei, Zhang Wei. Predictive value of MRI combined with serum lncRNA KCNQ1OT1, miR-204-5p for axillary lymph node metastasis of breast cancer [J]. Journal of International Oncology, 2025, 52(2): 89-93. |
| [12] | Yipala·Yilihamu , Ma Tao, Wang Yan, Gao Chunjie, Liu Jing, Zhao Ting, Wang Lei. Relationship between body mass indexes and survival prognosis of breast cancer patients with different menopausal status and molecular subtypes [J]. Journal of International Oncology, 2025, 52(12): 745-757. |
| [13] | Wu Huoyou, Wu Zujiao, Lin Sibo, Qu Yiyang. A predictive model for the efficacy of neoadjuvant chemotherapy in rectal cancer constructed based on multimodal MRI quantitative parameters [J]. Journal of International Oncology, 2025, 52(12): 770-776. |
| [14] | Zhao Biao, Zhu Yupu, Zhang Yating, Yuan Meifang, Li Han, Yang Yi, Sun Chaoxi. Study on dose optimization strategy of dynamic intensity-modulated radiotherapy based on the inner edge tangent field for the target area after breast-conserving surgery for left-sided breast cancer [J]. Journal of International Oncology, 2025, 52(11): 689-694. |
| [15] | Gao Wei, Zhang Ling, Wu Tianlei, Hu Lili, Rong Feng. A predictive model for radiation esophagitis in esophageal cancer patients based on machine learning [J]. Journal of International Oncology, 2025, 52(1): 31-37. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||